The dilemma? How do you as accurately as possible, anticipate, react to, and effectively plan for COVID-19 and similar epidemics? Let's carefully examine the data, because your likelihood of infection, treatment, and survival largely depends on where you live, the status of your health, and your race and gender.
THE GOOD - As far as U.S. citizens are concerned, if you're a minority or a poor person, you're not immediately likely to become a victim of the coronavirus (COVID-19), not because you're biologically immune, but because the overwhelming majority of persons exposed to "first contact" with COVID-19 are persons engaged in international travel, specifically to China, then Europe, and back to the United States with additional mobility. The overwhelming majority of Black people, other minorities, and poor White people do NOT have money to engage in international travel (dah) or frequent and discretionary domestic travel; and therefore, are least likely to be exposed to COVID-19. So, with regard to COVID-19, initially, being a minority and poor is a good thing.
It's also a good thing if you live in a state with excellent health care. As ranked in the 2019 America’s Health Rankings Annual Report by the United Health Foundation, the highest ranked states (i.e., best places to live for the "best" in health care) are presented below. The states are ranked according to a score derived from 35 measures across five categories of health: behaviors, community & environment, policy, clinical care and outcomes.
Highest Ranked States / Percent of White Residents (W) / Percent of Black Residents (B) Source: U.S. Census.gov
State
W
B
1.
Vermont
92.5
1.4
2.
Massachusetts
71.4
8.9
3.
Hawaii
21.8
2.2
4.
Connecticut
66.5
12.0
5.
Utah
78.0
1.4
6.
New Hampshire
90.0
1.7
7.
Minnesota
79.5
6.8
8.
New Jersey
54.9
15.0
9.
Washington
68.0
4.3
10.
Colorado
67.9
4.6
THE BAD - Sadly, as usual, the rich, the affluent (people with financial resources), and the powerful who are overwhelmingly White people, have much greater freedom to travel as they please, throughout the U.S. and throughout the world. This "practice" is nothing new. "The arrival of Europeans brought numerous diseases to the Americas, including smallpox, bubonic plague, chickenpox, cholera, the common cold, diphtheria, influenza, malaria, measles, scarlet fever, sexually transmitted diseases, typhoid, typhus, tuberculosis, and pertussis. Each of these brought destruction through sweeping epidemics, involving disability, illness, and extensive deaths. You'd be wrong to think that the richest and most powerul country in the world would have the best health care in the world.
According to the 2019 edition of the CEOWORLD magazine Health Care Index, which ranks 89 countries according to factors that contribute to overall health, Taiwan has the best health care systems in the world. A quick canvas of this list (below) reveals the United States ranked way, way behind (behind South Korea, Japan, Austria, Denmark, and more than two-dozen other nations at number thirty-(30). Equally bad, the United States is ranked #1 for spending the most on healthcare per capita according to the Organization for Economic Co-operation and Development (OECD). Given the dismal ranking for "quality of care," it truly cannot be said U.S. citizens are getting enough bang for their bucks. Additionally, as reported by Forbes.com, nations with the greatest success managing COVID-19 are often lead by women, notably in Denmark, Iceland, Finland, Germany, New Zealand, Norway, and Taiwan. Does gender matter? Of course not - unless, of course, you're one of the millions of U.S. citizens who still foolishly believe a woman could never effectively function as the highest level government official. Note the following exhibit.
Please note, India's population is over four-(4) times larger than the U.S., and throughout the pandemic, there have been three-(3) times fewer COVID-19 deaths in India (153,221 as of January 21, 2021) than in the U.S. (424,177 as of January 21, 2021). Please note, again, India has a "Best In Health Care" ranking of #19, conversely the United States of America has a ranking of #30. Do you really think the U.S. is the "pinnacle," the highest standard of health delivery in the world? By the way, as you consider the above data, keep in mind, individual nations, and individual States within the United States of America do NOT compile and report data consistently! Again, as you consider the above data, keep in mind, individual nations, individual states, counties, cities, etc., do NOT compile and report data consistently. For examples, click here and here and here and here, etc.
Some people believe "the problem" of the United States is its tradition of prioritizing individualism over government restrictions, or "States rights" versus the Federal Government overstepping its authority; and that this aversion to collective action helped lead to inadequate state lockdowns and inconsistent adherence to viable public health policies. Unfortunately, "individualism" in the United States is primarily centered on a hierarchy of race and sex, with White males (who represent on 30% of the U.S. population) on top of this pyramid; and ultimately, White males make the rules, and White males define all exceptions to the rules, and this hierarchy established and sustains health disparities.
So, here we are again, the rich and affluent, predominately White people, brought disease back to the U.S., which they spread to everyone else. As expected, COVID-19 has filtered down to the general public, to the social class of "worker bees." How exactly does the health and racial demographics of the working class reconcile to becoming victims of COVID-19, and does it matter? Let's connect the dots with the following exhibits.
By The New York Times | Sources: Oxford Covid-19 Government Response Tracker, New York Times database from state and local governments.
OBESITY - The rates of overweight or obesity for White men is 74.0 percent.
39% of non-Hispanic White women 40–59 years of age are obese.
RESPIRATORY - People at risk for COPD (Chronic obstructive pulmonary disease):
1. Women (37.4%).
2.
People aged 65 to 74 years and ≥75 years.
3.
American Indians/Alaska Natives and multiracial non-Hispanics.
3.
People who were unemployed, retired, or unable to work.
4.
People with less than a high school education.
5.
People who were divorced, widowed, or separated. Current or former smokers.
6.
People with a history of asthma.
7.
Lower socioeconomic status (SES) indicators such as educational attainment and income increase the risk of chronic lung diseases (CLDs) such as Chronic Obstructive Pulmonary Disease (COPD), emphysema, chronic bronchitis, and asthma.
Percentage (%) White People with Respiratory Disease, CDC
Emphysema
1.4
Ever has Asthma
13.5
Still has Asthma
7.5
Hay Fever
7.6
Sinusitis
11.7
Chronic Bronchitis
3.6
People 65 years and older*
People who live in a nursing home or long-term care facility
People with chronic lung disease or moderate to severe asthma
People who have serious heart conditions
People who are immunocompromised, including cancer treatment, smoking, bone marrow or organ transplantation, immune deficiencies, poorly controlled HIV or AIDS, and prolonged use of corticosteroids and other immune weakening medications
People with severe obesity (body mass index [BMI] of 40 or higher)
People with diabetes
People with chronic kidney disease undergoing dialysis
People with liver disease
* The Centers for Medicare & Medicaid Services report that in 2014, the most recent year for which data are available:
(a) 7.8% of nursing home residents were 95 years of age or older.
(b) 33.8% were 85 to 94 years old.
(c) 26.4% were 75 to 84 years old.
(d) 16.5% were 65 to 74 years old.
(e) 15.5% of the nursing home population is under age 65.
(f) women make up about two-thirds of the nursing home population (65.6%) (g) four of five nursing home residents (77.9%) are non-Hispanic whites
(h)
most have one chronic condition for which they need some ongoing medical care
NOTE: The novel coronavirus has claimed 16,231 American lives through April 9. However, data about the race and ethnicity of the deceased is available for just 35% of deaths.
5,700 Americans have died from COVID-19 as of Thursday, April 9, 2020.
42%
Forty-two-percent-(42%) of the people who have died are White as of Thursday, April 9, 2020.
For each 100,000 Americans (of their respective group), about 28 Whites have died from the coronavirus, a mortality rate similar to Asians (28), somewhat below Latinos (31) and Pacific Islanders (33), considerably below Indigenous people (43) and less than half of the rate experienced by Blacks (66).
UPDATE:
For this ethnic group per 100,000 persons, as of Thursday, June 23, 2020 28.5%
have died from the coronavirus.
OBESITY - The rates of overweight or obesity for Black men is 69.9 percent
82.1% of all adult Black women over 30 years of age are either morbidly overweight or obese.
57% of all adult Black women 40–59 years of age are obese.
61% of all adult Black women over 60 years of age are obese.
Black women have more than double the rates of extreme obesity as White and Hispanic women.
RESPIRATORY - People at risk for COPD (Chronic obstructive pulmonary disease):
1. Women (37.4%). 2.
People aged 65 to 74 years and ≥75 years.
3.
American Indians/Alaska Natives and multiracial non-Hispanics.
3.
People who were unemployed, retired, or unable to work.
4.
People with less than a high school education.
5.
People who were divorced, widowed, or separated. Current or former smokers.
6.
People with a history of asthma.
7. Lower socioeconomic status (SES) indicators such as educational attainment and income increase the risk of chronic lung diseases (CLDs) such as Chronic Obstructive Pulmonary Disease (COPD), emphysema, chronic bronchitis, and asthma.
Percentage (%) Black People with Respiratory Disease, CDC
Emphysema
1.1
Ever has Asthma
14.8
Still has Asthma
9.1
Hay Fever
5.5
Sinusitis
10.8
Chronic Bronchitis
3.4
Vitamin D deficiency -
Black Doctors sound the alarm
People 65 years and older*
People who live in a nursing home or long-term care facility
People with chronic lung disease or moderate to severe asthma
People who have serious heart conditions
People who are immunocompromised, including cancer treatment, smoking, bone marrow or organ transplantation, immune deficiencies, poorly controlled HIV or AIDS, and prolonged use of corticosteroids and other immune weakening medications
People with severe obesity (body mass index [BMI] of 40 or higher)
People with diabetes
People with chronic kidney disease undergoing dialysis
People with liver disease
* The Centers for Medicare & Medicaid Services report that in 2014, the most recent year for which data are available:
(a) 7.8% of nursing home residents were 95 years of age or older.
(b) 33.8% were 85 to 94 years old.
(c) 26.4% were 75 to 84 years old.
(d) 16.5% were 65 to 74 years old.
(e) 15.5% of the nursing home population is under age 65.
(f) women make up about two-thirds of the nursing home population (65.6%)
(g) four of five nursing home residents (77.9%) are non-Hispanic whites
(h) most have one chronic condition for which they need some ongoing medical care
NOTE: The novel coronavirus has claimed 16,231 American lives through April 9. However, data about the race and ethnicity of the deceased is available for just 35% of deaths.
34%
While BLACK Americans represent 13% of those living in places releasing data, they have suffered 34% of all known deaths as of April 9, 2020.
Across all the existing data, Black residents are 2.6 times more likely to die than we would expect based on their population. Most severely, in Michigan, Blacks are 3.8 times more likely to die of COVID-19 than their population share, and in Illinois, they are 3.3 times more likely to die. In Milwaukee County, Wisc., the ratio is 2.5, while the multiple of excess death among Black residents is in 2.4 in Chicago, and 2.2 in Louisiana. Of the eight states and four localities we examined, Minnesota is the only one that does not see a disproportionate mortality burden for its Black residents.
For each 100,000 Americans (of their respective group), about 66 Blacks have died from the coronavirus, a mortality rate more than double the rate for Latinos (31) and Pacific Islanders (33) and about 2.3 times the rate for Asians (28) and Whites (28). The overall Black mortality rate is 1.5 times as high as the Indigenous mortality rate, which is 43 per 100,000.
UPDATE:
For this ethnic group per 100,000 persons, as of Thursday, June 23, 2020 65.8%
have died from the coronavirus.
OBESITY - The rates of overweight or obesity for Hispanic men is 81.7 percent.
51% of Latino women 40–59 years of age are obese.
RESPIRATORY - People at risk for COPD (Chronic obstructive pulmonary disease): 1. Women (37.4%). 2.
People aged 65 to 74 years and ≥75 years.
3.
American Indians/Alaska Natives and multiracial non-Hispanics.
3.
People who were unemployed, retired, or unable to work.
4.
People with less than a high school education.
5.
People who were divorced, widowed, or separated. Current or former smokers.
6.
People with a history of asthma.
7. Lower socioeconomic status (SES) indicators such as educational attainment and income increase the risk of chronic lung diseases (CLDs) such as Chronic Obstructive Pulmonary Disease (COPD), emphysema, chronic bronchitis, and asthma.
Percentage (%) Latino People with Respiratory Disease, CDC
Emphysema
1.0
Ever has Asthma
11.5
Still has Asthma
6.0
Hay Fever
4.3
Sinusitis
8.0
Chronic Bronchitis
2.7
People 65 years and older*
People who live in a nursing home or long-term care facility
People with chronic lung disease or moderate to severe asthma
People who have serious heart conditions
People who are immunocompromised, including cancer treatment, smoking, bone marrow or organ transplantation, immune deficiencies, poorly controlled HIV or AIDS, and prolonged use of corticosteroids and other immune weakening medications
People with severe obesity (body mass index [BMI] of 40 or higher)
People with diabetes
People with chronic kidney disease undergoing dialysis
People with liver disease
* The Centers for Medicare & Medicaid Services report that in 2014, the most recent year for which data are available:
(a) 7.8% of nursing home residents were 95 years of age or older.
(b) 33.8% were 85 to 94 years old.
(c) 26.4% were 75 to 84 years old.
(d) 16.5% were 65 to 74 years old.
(e) 15.5% of the nursing home population is under age 65.
(f) women make up about two-thirds of the nursing home population (65.6%)
(g) four of five nursing home residents (77.9%) are non-Hispanic whites
(h) most have one chronic condition for which they need some ongoing medical care
NOTE: The novel coronavirus has claimed 16,231 American lives through April 9. However, data about the race and ethnicity of the deceased is available for just 35% of deaths.
16%
LATINOS experienced elevated mortality ratios only in New York state (1.3) and New York City (1.1), as of Thursday, April 9, 2020.
For each 100,000 Americans (of their respective group), about 31 Latinos have died from the coronavirus, a mortality rate slightly above Asians (28) and Whites (28), slightly below Pacific Islanders (33), and well below Indigenous people (43) and Blacks (66).
UPDATE:
For this ethnic group per 100,000 persons, as of Thursday, June 23, 2020 31.1%
have died from the coronavirus.
ASIAN
Rank
Causes of Death
(ICD-10)
1.
Malignant neoplasms
2.
Diseases of heart
3.
Cerebrovascular diseases
4.
Accidents (unintentional injuries)
5.
Diabetes mellitus
6.
Alzheimer disease
7.
Influenza and pneumonia
8.
Chronic lower respiratory diseases
9.
Nephritis, nephrotic syndrome and nephrosis
10.
Essential hypertension and hypertensive renal disease
OBESITY - Age-adjusted percentage of Asian persons 18 years of age and over who were obese, 2018 is 13% versus 30% for non-Hispanic White. (Body Mass Index (BMI) of 30 or greater). From 2004-2006, Filipino adults were 70 percent more likely to be obese as compared to the overall Asian population. About 1 in 10 Vietnamese and Korean adults were underweight, from 2004-2006.
Ethnicity
Overweight
Obese
All Asians
27.5
8.1
Chinese
21.8
4.2
Filipino
33.0
14.1
Asian Indian
34.4
6.0
Japanese
25.9
8.7
Vietnamese
19.1
5.3
Korean
27.3
2.8
Other
29.2
12.5
RESPIRATORY - People at risk for COPD (Chronic obstructive pulmonary disease):
1. Women (37.4%).
2.
People aged 65 to 74 years and ≥75 years.
3.
American Indians/Alaska Natives and multiracial non-Hispanics.
3.
People who were unemployed, retired, or unable to work.
4.
People with less than a high school education.
5.
People who were divorced, widowed, or separated. Current or former smokers.
6.
People with a history of asthma.
7. Lower socioeconomic status (SES) indicators such as educational attainment and income increase the risk of chronic lung diseases (CLDs) such as Chronic Obstructive Pulmonary Disease (COPD), emphysema, chronic bronchitis, and asthma.
Percentage (%) Asian People with Respiratory Disease, CDC
Emphysema
0.7
Ever has Asthma
7.8
Still has Asthma
3.7
Hay Fever
6.9
Sinusitis
6.6
Chronic Bronchitis
1.1
People 65 years and older*
People who live in a nursing home or long-term care facility
People with chronic lung disease or moderate to severe asthma
People who have serious heart conditions
People who are immunocompromised, including cancer treatment, smoking, bone marrow or organ transplantation, immune deficiencies, poorly controlled HIV or AIDS, and prolonged use of corticosteroids and other immune weakening medications
People with severe obesity (body mass index [BMI] of 40 or higher)
People with diabetes
People with chronic kidney disease undergoing dialysis
People with liver disease
* The Centers for Medicare & Medicaid Services report that in 2014, the most recent year for which data are available:
(a) 7.8% of nursing home residents were 95 years of age or older.
(b) 33.8% were 85 to 94 years old.
(c) 26.4% were 75 to 84 years old.
(d) 16.5% were 65 to 74 years old.
(e) 15.5% of the nursing home population is under age 65.
(f) women make up about two-thirds of the nursing home population (65.6%)
(g) four of five nursing home residents (77.9%) are non-Hispanic whites
(h) most have one chronic condition for which they need some ongoing medical care
NOTE: The novel coronavirus has claimed 16,231 American lives through April 9. However, data about the race and ethnicity of the deceased is available for just 35% of deaths.
4%
While Black Americans suffered unduly high deaths in nearly all places examined, ASIAN AMERICANS did so only in California, as of April 9, 2020. Across the state of California, Asians were 1.2 times more likely to die than their population share, and in Los Angeles County alone, Asian residents were 6.4 times more likely to die from the virus (although this represented only 18 deaths). Latinos experienced elevated mortality ratios only in New York state (1.3) and New York City (1.1).
For each 100,000 Americans (of their respective group), about 28 Asians have died from the coronavirus, a mortality rate similar to Whites (28), somewhat below Latinos (31) and Pacific Islanders (33), and well below the rates for Indigenous people (43) and Blacks (66).
UPDATE:
For this ethnic group per 100,000 persons, as of Thursday, June 23, 2020 27.7%
have died from the coronavirus.
OBESITY- American Indian/Alaska Native adolescents are 30 percent more likely than non-Hispanic white adolescents to be obese. American Indian or Alaska Native adults are 50 percent more likely to be obese than non-Hispanic whites.
Age-adjusted percentage of persons 18 years of age and over who were overweight but not obese, 2018.
33.1
Age-adjusted percentage of persons 18 years of age and over who were obese, 2018.
48.1
RESPIRATORY- People at risk for COPD (Chronic obstructive pulmonary disease):
1. Women(37.4%). 2.
People aged 65 to 74 years and ≥75 years.
3.
American Indians/Alaska Natives and multiracial non-Hispanics.
3.
People who were unemployed, retired, or unable to work.
4.
People with less than a high school education.
5.
People who were divorced, widowed, or separated. Current or former smokers.
6.
People with a history of asthma.
7. Lower socioeconomic status (SES) indicators such as educational attainment and income increase the risk of chronic lung diseases (CLDs) such as Chronic Obstructive Pulmonary Disease (COPD), emphysema, chronic bronchitis, and asthma.
Percentage (%) Asian People with Respiratory Disease,CDC
Emphysema
0.4
Ever has Asthma
14.9
Still has Asthma
9.5
Hay Fever
8.5
Sinusitis
10.5
Chronic Bronchitis
N/A
People 65 years and older*
People who live in a nursing home or long-term care facility
People with chronic lung disease or moderate to severe asthma
People who have serious heart conditions
People who are immunocompromised, including cancer treatment, smoking, bone marrow or organ transplantation, immune deficiencies, poorly controlled HIV or AIDS, and prolonged use of corticosteroids and other immune weakening medications
People with severe obesity (body mass index [BMI] of 40 or higher)
People with diabetes
People with chronic kidney disease undergoing dialysis
People with liver disease
* The Centers for Medicare & Medicaid Services report that in 2014, the most recent year for which data are available:
(a) 7.8% of nursing home residents were 95 years of age or older.
(b) 33.8% were 85 to 94 years old.
(c) 26.4% were 75 to 84 years old.
(d) 16.5% were 65 to 74 years old.
(e) 15.5% of the nursing home population is under age 65.
(f) women make up about two-thirds of the nursing home population (65.6%)
(g) four of five nursing home residents (77.9%) are non-Hispanic whites
(h) most have one chronic condition for which they need some ongoing medical care
NOTE: The novel coronavirus has claimed 16,231 American lives through April 9. However, data about the race and ethnicity of the deceased is available for just 35% of deaths.
TBD%
Insufficient data on NATIVE AMERICAN deaths related to the coronavirus, as of April 9, 2020.
For each 100,000 Americans (of their respective group), about 43 Indigenous people have died from the coronavirus, a mortality rate well above Whites (28), Asians (28), Latinos (31) and Pacific Islanders (33), although below the rates for Blacks (66).
UPDATE:
For this ethnic group per 100,000 persons, as of Thursday, June 23, 2020 43.2%
have died from the coronavirus.
As ranked in the 2019 America’s Health Rankings Annual Report by the United Health Foundation, the lowest ranked states (i.e., worst places to live for health care) are presented below. The states are ranked according to a score derived from 35 measures across five categories of health: behaviors, community & environment, policy, clinical care and outcomes.
Lowest Ranked States / Percent of White Residents (W) / Percent of Black Residents (B) Source: U.S. Census.gov
State
W
B
41.
Indiana
78.9
9.8
42.
South Carolina
63.7
27.1
43.
Kentucky
84.3
8.4
44.
Tennessee
73.7
17.1
45.
West Virginia
92.1
3.6
46.
Oklahoma
65.3
7.8
47.
Alabama
65.4
26.8
48.
Arkansas
72.2
15.7
49.
Louisiana
58.6
32.7
50.
Mississippi
56.5
37.8
THE VERY UGLY - Given the aforementioned facts, this is why the health and racial demographics of the "working class" directly reconciles to a linear alignment to victims of COVID-19, and yes, it does matter. Oh, yes, it matters. Given the aforementioned facts, there's overwhelming evidence the majority of Black people, other minorities, and poor White people already have the worst "health outcomes," which COVID-19 has yet again validated and amplified.
Socialism and communism are NOT the solution to the perpetual failure of the rich, the affluent, and the powerful to govern, legislate, or "humanely" manage capitalism. With regard to the health, safety, and well-being of every U.S. citizen, shouldn't egalitarian principles be "humanely" applied to every citizen, especially to the 80% of U.S. citizens who exist as "worker bees" and who live paycheck-to-paycheck? Consider the following:
A. As with HIV/AIDs and other previous and existing health related concerns, yet again, the rich, the affluent, and the powerful will continue to essentially ignore the planned and continued poor state of health of Black people and Native Americans (i.e., genocide); and ignore that COVID-19 has its most dire impact on Black people, other minorities, and poor White people, because the afforementioned: (1) have a much lower socioeconomic status; (2) the worst physical health; and (3) the least access to health care; and this is NOT going to change.
B. As validated by the enormous and perpetual wage gap between the overwhelming majority of U.S. citizens who live paycheck-to-paycheck and who are exploited by the rich, the affluent, and the powerful - the Occupational Safety and Health Administration (OSHA), Mine Safety and Health Administration (MSHA), Department of Energy (DOE), National Highway Traffic Safety Administration (NHTSA), etc., were not created as an act of altruism by the federal government and with support from business and industry, but not until after repeated injuries and deaths to employees and citizens. Case in point, the Triangle Shirtwaist Factory fire on March 25, 1911 that caused the deaths of 146 garment workers – 123 women and girls and 23 men – unable to escape from a locked building - who died from the fire, smoke inhalation, or falling or jumping to their deaths. Also, think about all the lives that could have been saved if cars were designed (we've had the technology for decades) to essentially eliminate accidents, injuries, and death. Unfortunately, the rich, the affluent, and the powerful erroneously believe such safety "benchmarks" would severely limit the financial eco-system of the property/casualty insurance industry, and car repair and service vendors, and parts and supply vendors, and all related financial components anchored to an authoritarian exploitation of capitalism. Here's a unique thought, a much better self-sustaining capitalist business paradigm: make money by building cars not anchored to overtly wasteful, environmentally unfriendly planned obsolescence; instead, design the perpetual innovation of recycling-based technology and safety; but this is NOT going to happen.
C. The Americans with Disabilities Act (ADA) was not created as an act of altruism by the federal government or with support from business and industry; the ADA was not created until after repeated acts of blatant workplace discrimination against people with physical and mental disabilities. Still, thirty-(30) years after the enactment of the ADA, people with disabilities are NOT routinely, if ever, considered for hire; and this is NOT going to change.
D. As reported by CareerBuilder.com, nearly 80% of U.S. workers live paycheck-to-paycheck, and due to the coronavirus, 6.6 million US workers filed for their first week of unemployment benefits in the week ending March 28, according to the Department of Labor — a new historic high! Clearly, if employers truly valued the emotional well-being of employees, the overwhelming majority of U.S. workers would not live paycheck-to-paycheck, and 6.6 million US workers (over 16+ million unemployment claims as of April 10, 2020) would not have filed for unemployment insurance, because the income gap between workers and senior management would be much, much less. Unfortunately, the overwhelming majority of U.S. workers will continue to live paycheck-to-paycheck, and this is NOT going to change.
To sustain the financial survival of 80% of U.S. workers ("citizens" and approved non-citizen taxpayers) who live paycheck-to-paycheck the government could have simultaneously required "designated" employers (employee groups, industries, etc.) to temporarily close and direct their employees to stay at home, while also requiring employers to submit weekly or monthly pay invoices to the IRS for subsequent direct deposit payments (stimulus checks) to employees. There would be no financial windfall for anyone, there would be no unemployment claims; a strategically orchestrated "plan" of financial sustenance to prevent "innocent" people from becoming homeless, starving, etc. It's just that simple. Instead your federal, state, county, or local governments . . .
1. Used the COVID-19 pandemic to unilaterally close small businesses, and without first securing approval (vote!) from citizens, and most importantly, without first establishing a viable means to sustain the financial survival of "citizens."
2. Used the COVID-19 pandemic to unilaterally close churches and other places of religion.
3. Used the COVID-19 pandemic to unilaterally and inappropriately enforce "police power," to terminate, amend, abridge, and supersede legally executed civil contracts and work-for-hire agreements YOU establsihed with creditors, vendors, and clients, and again, without first establishing a viable means to sustain the financial survival of "citizens."
FACT: Again, nearly 80% of U.S. workers live paycheck-to-paycheck, but the COVID-19 pandemic has not jeopardized the "perpetual employment and perpetual income" of members of the U.S. Congress, and other government officials. QUESTION: Is it "fair" for people who are not at risk of losing their jobs or income to unilaterally determine the "fate" of regular citizens who actually have to work for a living?
Instead of closing businesses and schools, and generating measly stimulus checks, and in anticipation of another pandemic, why didn't YOUR federal, state, county, and local governments create an "economic boom" by funding the renovation or construction of a sustainable pandemic infrastructure? As represented by the illustration below, why didn't YOUR government develop viable strategies that simultaneously ensure public health AND sustain economic development? Why??
Clearly, there could have been, would have been an "economic boom" if your government had acted to fast track the robust creation of "Made in the USA" PPEs, infrastructure renovation or construction, upgrades to or installation of ASHRAE certified HVAC systems, and the design and adoption of related public and private sector strategies to protect public health AND to sustain economic development.
5. Used the COVID-19 pandemic to unilaterally define if, when, and where you can peaceably assemble - even in your own homes and/or places of business, and to unilaterally define how many individuals can assemble. (Psst! You really, really, really need to read"1984" by George Orwell; or at least see the movie; or watch this "live" theatre performance of "The Obsolete Man" from the original "The Twilight Zone."
E. The rich, the affluent, and the powerful know that every year, as the suns rises and sets, in certain geographic areas we can expect earthquakes, wildfires, hurricanes, tornadoes, etc. Every year. Nevertheless, it remains the practice of the rich, the affluent, and the powerful to build homes, schools, and businesses that are not designed to survive environmental catastrophes. Even worse, despite having the technology and financial resources to significantly reduce or eliminate constantly reoccurring environmental destruction and loss of life (as represented below in the pictures of levees in the Netherlands and London), the United States of America incurs the same great loss of property and loss of life over and over, year after year. Equally distrubing, the rich, the affluent, and the powerful use laws and commerce to inhumanely propel their minions of "worker bees" to live and work where structures have not been designed to survive environmental catastrophes. That's just stupid, if not insane. Albert Einstein said it so clearly, “Insanity: Doing the same thing over and over again and expecting different results.” Sadly, even with additional property loss and loss of life, the U.S. is NOT going to change.
Netherlands
London
New Orleans
Pandemic Pollution: Plastic & PPE Pileup
F. As reported by CBS News and hundreds of print and broadcast media, health care workers and citizens do not have enough personal protective equipment (PPE) to protect themselves from COVID-19. Sadly, the overwhelming majority of PPEs and related supplies are not produced in the United States but in China and elsewhere, because the very narcissistic-get-rich paradigm of the rich, the affluent, and the powerful intentionally killed manufacturing of PPEs in the U.S. and eliminated millions of U.S. jobs by exporting PPE manufacturing overseas. Although the United States is the world's second largest manufacturer (after China), manufacturing employment has been declining since the 1990s, and as of 2018, manufacturing contributed less to GDP than the 'finance, insurance, real estate, rental, and leasing' sector, the 'government' sector, or the 'professional and business services' sector. Isn't it sad, ironic, and pathetic the U.S. must order PPEs from the country, China, where COVID-19 originated? Plus, given the traditionally high rates of unemployment with Black men, steel industry workers, coal and mining industry workers, and people in the service, retail, and trucking and transportation industries who continue to lose their jobs to automation and advances in technology, why haven't the rich, the affluent, the powerful exploited this pool of underutilized and available human capital? Sadly, it remains the business paradigm of the rich, the affluent, and the powerful to increase thewage gap, keep salaries and income of "worker bees" low, and this is NOT going to change.
G. Although there's plenty of business, political, medical, and scientific acumen throughout every aspect of this United States of America, sadly, in perpetual abeyance is: (1) simple common sense; and (2) the means and opportunity to "act" on common sense. Case in point, after you watch the following five-(5) videos you'll likely realize, there are better ways to "manage" COVID-19, but . . .
. . . consistency in thought and practice is NOT going to happen, especially from the perpetually contradictory mouth of the nation’s top infectious-diseases expert and chief medical adviser to President Biden, Dr. Anthony Fauci and many of this contemporaries.
Source: nypost.com - So let’s start by being brutally honest about Dr. Anthony Fauci, who has been the source of some of the most damaging misinformation about COVID-19.
At the very least, the nation’s top infectious diseases expert and chief medical adviser to Biden is loose with the facts and is prone to changing his mind. This is the man who dictated coronavirus policy in the Trump administration. If mistakes were made, as the Biden administration claims, they are Fauci’s. Yet, astonishingly, Fauci told CNN Friday that a “lack of candor” from the Trump administration had cost American lives. If people’s lives really were at stake last year, why did he wait until now to tell us? Chalk it up to another convenient fib from a habitual fibber, who has deceived us on everything from masks to herd immunity.
Dr. Duc Vuong, World's #1 Weight Loss Surgeon
Author of 13 books, explains how
coronavirus kills its victims
Dr. SHIVA Ayyadurai, MIT PhD
Crushes Dr. Fauci Exposes Birx, Clintons,
Bill Gates, and The W.H.O
IS IT TRUE WEARING MASKS FOR
EXTENDED PERIODS OF TIME IS OKAY?
COVID 19: Does wearing a mask really help,
and what's the downside?
COMMON SENSE QUESTION: IF MASKS DON'T IMPAIR BREATHING,
HOW COME ATHLETES DON'T WEAR MASKS WHILE COMPETING?
COMMON SENSE RESPONSE: MASKS CLEARLY IMPAIR BREATHING, AND
RESTRICT THE NATURAL EXCHANGE OF OXYGEN AND CARBON DIOXIDE.
Danika Bueno, BSN” (Bachelor of Science in Nursing)
If you disagree, read the fact check, here.
Dozens in Central Florida contract COVID-19 after being fully vaccinated
COVID-19 requires everyone to be safe, but not stupid. Humans are designed to primarily breathe through our noses, not our mouth. Plus, as runners know, it's STUPID to "recycle" your own air, to re-breathe your CO2, because your muscles atrophy due to lack of oxygen. Again, please be safe, protect yourself and others, practice social distancing, and as much as possible, try to exist in areas with adequate ventilation.
Do stricter health measures or requirements work?
There's no overwhelming evidence that
stricter health measures are better than doing nothing at all.
There's no overwhelming evidence that
stricter health measures are better than doing nothing at all.
Before a potential treatment reaches the clinical trial stage, scientists research ideas in what is called the discovery phase. This step can take from three to six years. Typically, researchers will test a potential new treatment in animals before moving on to the first stage of clinical testing in humans.
Phase 1: These trials usually enroll 20 to 100 healthy volunteers or people with the condition being studied, and last several months. This phase measures safety by testing for any adverse side effects of the treatment, but not necessarily how effective the drug or device is.
Phase 2: Around 70% of potential new drugs enter Phase 2, which continues to measure safety, while also looking at how effective the treatment is and carefully investigating its side effects. Phase 2 trials recruit up to several hundred patients with the condition to take part. This phase typically lasts several months to two years.
Phase 3: Just 33% of drugs make it to Phase 3, which tests the potential treatment in the largest number of people. This phase measures both safety and effectiveness with many volunteers, sometimes thousands. Phase 3 trials last from one to four years. FDA approval: After Phase 3, a pharmaceutical company may submit a New Drug Application (NDA) or a biologics license application (BLA) for the treatment to the Food and Drug Administration (FDA). The FDA then reviews results from all stages of the trial to determine whether it will approve the drug and allow the pharmaceutical company to begin marketing it to the public.
Phase 4: This phase is often called “Post-Approval Research and Monitoring.” After a new treatment is approved by the FDA, the pharmaceutical or device company may want to continue monitoring patients to learn more about the treatment’s longer-term effects, while comparing it against other already-approved options. It may take time for long-term side effects to appear, making this an important phase.
The clinical trial process is long — and it's set up that way so that by the time drugs reach the public, they have been thoroughly evaluated. But the length of the process is one reason why it's so important for volunteers to take part. Without enough volunteers, up to 80% of clinical trials are delayed.
Additionally, the CDC and FDA established the Vaccine Adverse Event Reporting System (VAERS) in 1990. The goal of VAERS, according to the CDC, is “to detect possible signals of adverse events associated with vaccines.” (A signal in this case is evidence of a possible adverse event that emerges in the data collected.) About 30,000 events are reported each year to VAERS. Between 10% and 15% of these reports describe serious medical events that result in hospitalization, life-threatening illness, disability, or death.
Is there money to be made? Absolutely. As reported by Visual Capitalist, in 2020, the world’s 50 largest pharmaceutical companies combined for an enormous $851 billion in revenues. However, there's nothing wrong with people making money based on the business model of using science and technology to improve the health and wellbeing of people. Unfortunately, Big Pharma lost a bunch of money due to the opiate crisis, but fortunately Big Pharma has been able to recoup its losses and make even more money via the COVID-19 pandemic.
Top five biggest pharmaceutical companies in the world by market capitalization
1. Johnson & Johnson - The pharmaceutical and consumer goods giant is worth $428.7 billion in market cap. They developed the third vaccine authorized for use in the U.S. and were named among the TIME100 Most Influential Companies List in 2021.
2. Roche - The Swiss pharmaceutical giant is at the forefront of oncology, immunology, infectious diseases, ophthalmology, and neuroscience. In 2019, Roche’s pharma segment sales rose by a healthy 16% to $53 billion.
3. Pfizer - Despite being the leading COVID-19 vaccine manufacturer in North America, Pfizer slid in the rankings to third place. The company has recently gained momentum, especially in the past quarter, with Q2’2021 revenues of $19.0 billion, reflecting a 86% operational growth from 2020.
4. Eli Lilly - Eli Lilly has taken a significant step towards establishing itself as a pharmaceutical industry leader. Having a market cap value of $125 billion in 2019, Eli Lilly has jumped to a current value of $214.9 billion, a significant growth of 72%.
5. Novartis - The second-biggest pharmaceutical company out of Switzerland, Novartis has been the face of the pharma industry for about 25 years. The primary manufacturer for the most recognizable drugs on the market pulled in a revenue of over $48 billion in 2020, a 3% increase compared to 2019.
RANK
COMPANY NAME
MARKET CAP VALUE
COUNTRY
1
Johnson & Johnson
$428.66 B
USA
2
Roche
$320.41 B
Switzerland
3
Pfizer
$219.39 B
USA
4
Eli Lilly
$208.99 B
USA
5
Novartis
$207.70 B
Switzerland
6
AbbVie
$202.60 B
USA
7
Merck
$191.67 B
USA
8
Novo Nordisk
$187.83 B
Denmark
9
Astrazeneca
$152.28 B
UK
10
Bristol-Myers Squibb
$145.80 B
USA
11
Amgen
$136.50 B
USA
12
Sanofi
$130.37 B
France
13
CVS Health
$110.49 B
USA
14
GlaxoSmithKline
$104.30 B
UK
15
CSL
$103.10 B
Australia
16
Gilead Sciences
$83.62 B
USA
17
Moderna
$83.25 B
USA
18
Merck KGaA
$80.61 B
Germany
19
Bayer
$59.43 B
Germany
20
Jiangsu Hengrui Medicine
$58.51 B
China
Given the aforementioned, what is the character and scope of a typical "Big Pharma" business model to use science and technology to manage or eliminate COVID-19, and thereby improve the health and wellbeing of people. Consider the public disclosure, presented below, in GSK's 2020 Annual Report..
GlaxoSmithKline (GSK) is a British multinational pharmaceutical company headquartered in London, England. Established in 2000 by a merger of Glaxo Wellcome and SmithKline Beecham, GSK was the world's sixth largest pharmaceutical company according to Forbes as of 2019, after Pfizer, Novartis, Roche, Sanofi, and Merck & Co. GSK is the tenth largest pharmaceutical company and #296 on the 2019 Fortune 500, ranked behind other pharmaceutical companies including China Resources, Johnson & Johnson, Roche, Sinopharm, Pfizer, Novartis, Bayer, Merck, and Sanofi.
In 2012, under prosecution by the United States Department of Justice (DoJ) based on combined investigations of the Department of Health and Human Services (HHS-OIG), FDA and FBI, primarily concerning sales and marketing of the drugs Avandia, Paxil, and Wellbutrin, GSK pleaded guilty to promotion of drugs for unapproved uses, failure to report safety data, and kickbacks to physicians in the United States and agreed to pay a US$3 billion (£1.9bn) settlement. It was the largest health-care fraud case to date in the US and the largest settlement by a drug company. Source: Wikipedia
Is a vaccine safe? Seriously, is it really safe?
Dr. Peter McCullough explains "everything!" WATCH THIS VIDEO!
Except for COVID-19, it's an accepted medical practice for a patient to get a "second opinion,"
due to inconsistencies and disputes within and between scientists and doctors on the efficacy medical treatment. WHY IS COVID-19 AN EXCEPTION?
Except for COVID-19, it's an accepted medical practice for a patient to get a "second opinion,"
due to inconsistencies and disputes within and between scientists and doctors on the efficacy medical treatment. WHY IS COVID-19 AN EXCEPTION?
Woman Dies 4 days after getting COVID Vaccine | Post Vaccine Deaths
OBSERVATION: Only after the second COVID-19 shot was it necessary for a 39-year-old single mom Kassidi Kurill, to take acetaminophen. If Kurill had not taken acetaminophen would she not have become gravely ill? We don't know know, no one knows, because there are absolutely no long-term research studies to validate the safety of any of the COVID-19 vaccines in reaction to Trigeminal Neuralgia and Botox. Does Kurill's daughter think the COVID-19 vaccine was worth the risk of her mother's death?
While Pfizer pharmaceutical had made headlines on the release of their Coronavirus vaccine, a former Vice President and Chief Scientist of the company Dr. Michael Yeadon has said that there is no need for any vaccines to bring the COVID-19 pandemic to an end. According to an article published in Lockdown Sceptics, Dr. Michael Yeadon wrote, “There is absolutely no need for vaccines to extinguish the pandemic. I’ve never heard such nonsense talked about vaccines. You do not vaccinate people who aren’t at risk from a disease. You also don’t set about planning to vaccinate millions of fit and healthy people with a vaccine that hasn’t been extensively tested on human subjects.”
Mount Vernon school board meeting with Dr Dan Stock
As you watch the rebuttal (fact check) below, ask yourself the following questions:
1. Why does the rebuttal ignore the fact the overwhelming majority of "consumer" masks are not N95, but simply cloth or paper masks?
2. Why does the rebuttal ignore the fact the overwhelming majority of COVID-19 victims are morbidly overweight and obese, and that a more pragmatic and long-term solution would be to pursue weight reduction, wellness, better nutrition, and fitness initiatives?
3. Perhaps, due to their own professional jealously, why did the "experts" refute Dr. Stock's success with Ivermectin, Vitamin D, and Zinc without actually validating "his" results? FACT: Just because treatments are not approved by the CDC or WHO does not mean they don't work!
he over
The COVID-19 vaccine is NOT a cure, it does not make you immune (at best it's only a "treatment"), and it requires frequent booster shots because its effectiveness wanes!
FACT: There’s no cure for the common cold, the best thing you can do is ease the symptoms. Over-the-counter (OTC) drugs can help with many different symptoms. However, you likely won’t experience all possible symptoms of the cold during every cold you have. The drug that you choose will depend on your specific symptoms.
FACT: There’s no cure for COVID-19, the best thing you can do is: (a) improve your immune system to hopefully avoid COVID-19 or ease the symptoms if you become infected; (b) if infected with the disease, your body subsequently produces its own antibodies to heal and protect you; and (c) take one of several vaccines that do NOT make you immune to COVID-19 or prevent you from passing the disease on to others, but the vaccines do ease the symptoms of the disease.
As detailed below, there's a big difference between taking time to carefully create a vaccine that actually establishes an immunity, versus creating a short-term fix with extremely limited therapeutic value.
SMALLPOX - Smallpox vaccination provides full immunity for 3 to 5 years and decreasing immunity thereafter. If a person is vaccinated again later, immunity lasts even longer. Historically, the vaccine has been effective in preventing smallpox infection in 95% of those vaccinated. To stay protected from smallpox, you should get booster vaccinations every 3 years. Thanks to the success of vaccination, the last natural outbreak of smallpox in the United States occurred in 1949. In 1980, the World Health Assembly declared smallpox eradicated (eliminated), and no cases of naturally occurring smallpox have happened since.
CHILDREN - CDC recommends all children get two doses of MMR (measles-mumps-rubella) vaccine, starting with the first dose at 12 through 15 months of age, and the second dose at 4 through 6 years of age. Children can receive the second dose earlier as long as it is at least 28 days after the first dose.
ADULTS - Adults should also be up to date on MMR vaccinations with either 1 or 2 doses (depending on risk factors) unless they have other presumptive evidence of immunity to measles, mumps, and rubella. One dose of MMR vaccine, or other presumptive evidence of immunity, is sufficient for most adults.
That's right, you'll need at least two-(2) to four-(4) shots in less than a year to "handle, but not cure" COVID-19, because the effectiveness of the vaccination wanes and does not create an immunity! The U.S. will recommend most Americans get a COVID-19 booster dose eight months after receiving their second shot, sources familiar with the planning process told The New York Times Aug. 16. Four things to know about the plan:
1. White House officials told The New York Times the U.S. is planning to announce its booster plan as early as this week. They also said booster doses could be offered as soon as mid-September.
2. The announcement will let Americans who received Pfizer's or Moderna's vaccine know they will need additional protection against coronavirus variants. The sources told The New York Times Americans who received Johnson & Johnson's one-dose vaccine will also likely need an additional dose, but the U.S. is waiting for the drugmaker to produce results for its clinical trial testing a two-dose regimen.
3. The plan is contingent upon FDA approval for COVID-19 boosters, which hasn't been granted yet. The agency amended the emergency use authorizations for Pfizer's and Moderna's COVID-19 vaccines Aug. 12, allowing for a third dose in immunocompromised people, but not yet for the rest of the population.
4. The booster plan for the rest of the population will likely follow a priority framework similar to the one employed during the country's initial vaccine rollout. Nursing home residents and healthcare workers will likely be the first groups eligible to receive booster shots, followed by Americans age 65 and older.
Dr. Michael Yeadon commented, “SAGE says everyone was susceptible and only 7% have been infected. I think this is literally unbelievable. They have ignored all precedent in the field of immunological memory against respiratory viruses. They have either not seen or disregarded excellent quality work from numerous, world-leading clinical immunologists which show that around 30% of the population had prior immunity.” “They should also have excluded from ‘susceptible’ a large subset of the youngest children, who appear not to become infected, probably because their immature biology means their cells express less of the spike protein receptor, called ACE2. I have not assumed all young children don’t participate in transmission, but believe a two thirds value is very conservative. It’s not material anyway,” Yeadon wrote “So SAGE is demonstrably wrong in one really crucial variable: they assumed no prior immunity, whereas the evidence clearly points to a value of around 30% (and nearly 40% if you include some young children, who technically are ‘resistant’ rather than ‘immune’),” wrote Yeadon and considering the reality of herd immunity, when susceptibility to a virus falls this low, at around 28 to 35%, “that population can no longer support an expanding outbreak of disease,” and thus the virus “wanes and disappears.”
“The pandemic is effectively over and can easily be handled by a properly functioning NHS (National Health Service). Accordingly, the country should immediately be permitted to get back to normal life.” concludes Yeadon.
5 pharmacy execs respond to vaccinated patients' worries they're no longer protected against COVID-19
Amir Emamifar, PharmD. Chief Pharmacy Officer at Temple University Health System (Philadelphia). Immunity is a multi-factorial and it is not just about the number of antibodies to a specific virus that you have in your bloodstream. So, there’s no easy way to measure if your immunity to COVID-19 is fading, particularly if you’re healthy. New research indicates that the protection the two mRNA vaccines (Pfizer and Moderna) create against COVID-19 might fade after several months.
Joel Hennenfent, PharmD. Chief Pharmacy Officer at Truman Medical Centers (Kansas City, Mo.). It is important to share that fully vaccinated patients are still safe. Emerging data shows fully vaccinated patients are still well protected from severe illness, hospitalization and death from COVID-19. It is important for those that are immunocompromised, as defined by the CDC, to receive a third dose to achieve the same degree of protection as those who are not immunocompromised. The thought behind a "booster for all" approach in the coming months is to try to get ahead of the possible downstream effects of the Delta variant and waning immunity against mild and moderate infections that can occur with time.
Kuldip Patel, PharmD. Senior Associate Chief Pharmacy Officer at Duke University Health System (Durham, N.C.). While it is true that vaccine efficacy wanes over time, this is not a new development. Most vaccines have a window of time during which they provide us the immunoprotection from the respective infection or disease. Booster doses and schedules for the COVID-19 vaccines are developed similarly to how other vaccine schedules have been developed, to ensure that we maintain and prolong the immunoprotective effects of the vaccine when it begins to wane. Not doing so will undoubtedly increase the risk of contracting the infection.
Tim Lynch, PharmD. Chief Pharmacy Officer at Multicare Health System (Tacoma, Wash). The COVID-19 pandemic is an evolving situation and we continue to learn more about newer variants and how best to adapt our response. While the goal of vaccine development was to fully protect against COVID-19 infection from the novel coronavirus and potential variants, the reality is that like most other vaccines, it is not fully effective in preventing vaccinated patients from becoming infected.
Linda Tyler, PharmD. Clinical Professor at the University of Utah's College of Pharmacy and former Chief Pharmacy Officer at University at Utah Health (Salt Lake City). When the COVID-19 vaccines were first available, we knew a two-dose series of the Pfizer or Moderna vaccines (one dose for the Johnson & Johnson vaccine) would be needed to provide the best protection against COVID-19. What we didn’t know is how long that protection would last. Researchers were carefully monitoring this. We now know that our protection starts to decrease at about 6-8 months.
Why is there no consistency in the treatment of COVID-19?
QUESTION:Which drugs are you using most frequently to treat your COVID-19 patients?
Sanjana Koshy, MD, infectious diseases physician at Mount Sinai (New York City): We recommend dexamethasone for all our hospitalized patients requiring supplemental oxygen. This was based on the RECOVERY trial that showed a survival benefit in patients on supplemental oxygen. We have increasingly used tocilizumab in combination with dexamethasone in our severely ill hospitalized patients with rapidly increasing oxygen requirements. We continue to use remdesivir for our hospitalized patients on low-flow oxygen. We are also glad to be able to offer the monoclonal antibody therapy casirivimab/imdevimab as treatment for select nonhospitalized patients who are at risk for severe COVID-19. This treatment is now also available as post-exposure prophylaxis for patients recently exposed to COVID-19 infection and at risk for severe disease, hospitalization and death.
Thomas Lew, MD, clinical assistant professor of medicine at Stanford University in California: We use the medications with the best data and outcomes. For hypoxic patients, dexamethasone and remdesevir, if within a 10-day window of symptom onset. In addition, if they become more severely hypoxic, in select groups of patients, we will give them immune modulators such as tocilizumab or baricitinib. We also usually place patients on prophylactic enoxaparin given the increased thrombotic risk during COVID-19 infections.
Marc Sala, MD, pulmonary and critical care physician at Northwestern Medicine (Chicago): Three drugs remain the backbone of my strategy against acute COVID-19 infection. I use monoclonal antibodies for outpatients that are at risk of severe disease and dexamethasone and remdesivir for my patients who are hospitalized in the ICU.
Daniel Solomon, MD, infectious diseases physician at Brigham and Women’s Hospital (Boston): For patients who are sick enough to be hospitalized and require oxygen, we are using the antiviral remdesivir, along with corticosteroids such as dexamethasone. Some patients who are severely ill benefit from an additional immunosuppressive drug, such as tocilizumab or baricitinib. For patients who have COVID-19 in the outpatient setting, our treatment options remain somewhat limited. Individuals who are at high risk for progression to severe disease can be given monoclonal antibody therapy that decreases the risk of hospitalization and death. There is some preliminary data to suggest an inhaled steroid called budesonide may be helpful, and some early studies that indicate an antidepressant drug called fluvoxamine may be beneficial, but we are awaiting more data on these treatments at this time, and they are not being used as standard of care.
Daniel Sterman, MD, director of the division of pulmonary medicine and critical care at NYU Langone Health (New York City): Dexamethasone, low-molecular weight heparin, remdesivir, tocilizumab and baricitinib.
Tara Vijayan, MD, infectious diseases physician at UCLA Health (Los Angeles): For outpatients, a combination monoclonal antibody therapy (casirivimab/imdevimab) for our patients at highest risk of hospitalization. For inpatients, a monoclonal antibody therapy if not hypoxic; dexamethasone if hypoxic. We do give five days of remdesivir if they have had fewer than 14 days of symptoms. If patients are not responding to steroids and are worsening [worsening oxygen needs] we consider baricitinib if they are on what we call high-flow nasal cannula, or tocilizumab if they are in the ICU. We have had a shortage of tocilizumab, so we have considered using sarilumab in lieu of this, based on limited data.
QUESTION: Which drugs are you avoiding?
Dr. Koshy: We avoid drugs for which there is insufficient evidence for use in COVID-19, unless it is within the context of a clinical trial. We believe that vaccination is key to control of the pandemic. Vaccination is very effective in protecting our patients and our families from severe COVID-19. We strongly encourage everyone age 12 and up to be fully vaccinated, and we are offering a third dose to people who are immunocompromised.
Dr. Lew: We are avoiding medications with no proven benefit at this time, including hydroxychloroquine, ivermectin, high-dose vitamin C and zinc.
Dr. Sala: Azithromycin, hydroxychloroquine and ivermectin. They are distractions in the real fight.
Dr. Solomon: We are avoiding the use of medications that have limited data or have plenty of data that does not show any benefit. Medications that have been tested and not been shown to be effective include hydroxychloroquine, lopinavir/ritonavir, colchicine and ivermectin. Importantly, we are also avoiding oral corticosteroids for patients who are in the outpatient setting, as this can lead to worse outcomes. We typically reserve steroid use for patients who are sick enough to be hospitalized unless there is another indication for the use of steroids, such as a COPD exacerbation.
Dr. Sterman: Hydroxychloroquine, azithromycin, ivermectin, vitamin C, vitamin D and zinc.
Dr. Vijayan: We do not recommend ivermectin or azithromycin at this time in the outpatient setting. We absolutely avoid steroids if patients are not hypoxic.
QUESTION: Which do you find most effective in treating your patients? Can you give your top 3?
Dr. Koshy:Steroids — dexamethasone continues to remain the most effective treatment for patients requiring supplemental oxygen. In patients with rapidly escalating oxygen requirements, we are seeing some benefit with the addition of tocilizumab. Additionally, the increasing availability and early utilization of casirivimab/imdevimab in nonhospitalized patients is likely contributing to preventing hospitalizations for COVID-19.
Dr. Lew:The most effective treatments tend to be oxygen, time and supportive care. But medication-wise, the most effective drugs tend to be dexamethasone, remdesivir, and in select patients, tocilizumab.
Dr. Sala:The most effective strategy to prevent COVID-19 is to vaccinate, but if a COVID-19 patient is in the ICU, use pronation, which means lying face-down, and administer dexamethasone.
Dr. Solomon:The combination of remdesivir and dexamethasone has been effective for our patients who are hospitalized. Monoclonal antibody therapy is the most effective available treatment for eligible patients who are in the outpatient setting, although the route of administration (IV infusion) is sometimes a logistical barrier. Of the agents currently under investigation, fluvoxamine has shown the most promise for outpatient treatment, but we are still awaiting more clinical data to help guide its use.
Dr. Sterman:Dexamethasone, low-molecular weight heparin and remdesivir.
Dr. Vijayan:Steroids (dexamethasone) if patients are hypoxic. Monoclonal antibodies if patients are not hypoxic. Possibly tocilizumab for patients who are progressing on steroids.
In summary, there's absolutely no consensus on how best to treat COVID-19, but we're supposed to believe a collection of "one size fits all vaccines," all with no long-term studies to validate safety and efficacy, is the best "treatment" for everyone? Really?
NEWS FLASH: NCAA rules COVID-19 infection is considered the equivalent of "fully vaccinated."
The NCAA has released updated guidance for winter sports competing during the COVID-19 pandemic.
The 2022 Winter Training and Competition document (PDF) follows recent updates by the Centers for Disease Control and Prevention, including recommendations for quarantine and isolation. The updated guidance addresses broad considerations that differentiate COVID-19 management in Tier 1 individuals based on vaccination and other immunity considerations.
For purposes of the winter guidelines, the NCAA COVID-19 Medical Advisory Group has developed a definition of "fully vaccinated" that considers both vaccination status and other immunity factors that may impact risks for Tier 1 individuals, including student-athletes and coaches. Those considered fully vaccinated include people:
Within two months of having completed the primary series of the Johnson & Johnson vaccine (one dose).
Within five months of having completed the primary series of the mRNA Pfizer vaccine, or within six months of having completed the primary series of the mRNA Moderna vaccine (two doses for both).
Who have received a booster vaccine if they are beyond two months of the Johnson & Johnson vaccine or beyond five or six months of the mRNA Pfizer or Moderna vaccine, respectively.
A person who has had a documented COVID-19 infection in the past 90 days is considered the equivalent of "fully vaccinated."
The "Tuskegee Syphilis Study," was an ethically unjustified study conducted continuously between 1932 and 1972 by the United States Public Health Service (PHS) and the Centers for Disease Control and Prevention (CDC). The purpose of this study was to observe the natural history of untreated syphilis. Although the African-American men who participated in the study were told that they were receiving free health care from the federal government of the United States, they were not.
The Public Health Service started the study in 1932 in collaboration with Tuskegee University (then the Tuskegee Institute), a historically black college in Alabama. In the study, investigators enrolled a total of 600 impoverished African-American sharecroppers from Macon County, Alabama. Of these men, 399 had latent syphilis, with a control group of 201 men who were not infected. As an incentive for participation in the study, the men were promised free medical care, but were deceived by the PHS, who never informed subjects of their diagnosis and disguised placebos, ineffective methods, and diagnostic procedures as treatment.
The men were initially told that the "study" was only going to last six months, but it was extended to 40 years. After funding for treatment was lost, the study was continued without informing the men that they would never be treated. None of the infected men were treated with penicillin despite the fact that by 1947, the antibiotic was widely available and had become the standard treatment for syphilis. The study continued, under numerous Public Health Service supervisors, until 1972, when a leak to the press resulted in its termination on November 16 of that year. The study caused the deaths of 128 of its participants, either directly from syphilis or from related complications.
The 40-year Tuskegee Study was a major violation of ethical standards, and has been cited as "arguably the most infamous biomedical research study in U.S. history." Its revelation led to the 1979 Belmont Report and to the establishment of the Office for Human Research Protections (OHRP) and federal laws and regulations requiring institutional review boards for the protection of human subjects in studies involving them. The OHRP manages this responsibility within the United States Department of Health and Human Services (HHS). Its revelation has also been an important cause of distrust in medical science and the US government amongst African Americans.
On May 16, 1997, President Bill Clinton formally apologized on behalf of the United States to victims of the study, calling it shameful and racist. "What was done cannot be undone, but we can end the silence," he said. "We can stop turning our heads away. We can look at you in the eye, and finally say, on behalf of the American people, what the United States government did was shameful and I am sorry."
The 40-year Tuskegee Study was a major violation of ethical standards, and has been cited as "arguably the most infamous biomedical research study in U.S. history." Its revelation led to the 1979 Belmont Report and to the establishment of the Office for Human Research Protections (OHRP) and federal laws and regulations requiring institutional review boards for the protection of human subjects in studies involving them. The OHRP manages this responsibility within the United States Department of Health and Human Services (HHS). Its revelation has also been an important cause of distrust in medical science and the US government amongst African Americans.
On May 16, 1997, President Bill Clinton formally apologized on behalf of the United States to victims of the study, calling it shameful and racist. "What was done cannot be undone, but we can end the silence," he said. "We can stop turning our heads away. We can look at you in the eye, and finally say, on behalf of the American people, what the United States government did was shameful and I am sorry."
Oh, but there's more . . .
During an 1835 trip to the United States, French visitor Harriet Martineau found that Black people lacked the power even to protect the graves of their dead. "In Baltimore the bodies of coloured people exclusively are taken for dissection," she remarked, "because the Whites do not like it, and the coloured people cannot resist."'l Four years later, abolitionist Theodore Dwight Weld echoed Martineau's sentiment. "Public opinion," he wrote, "would tolerate surgical experiments, operations, processes, performed upon them [slaves], which it would execrate if performed upon their master or other whites."1' Slaves found themselves as subjects of medical experiments because physicians needed bodies and because the state considered them property and denied them the legal right to refuse to participate.
And more . . .
Two antebellum experiments, one carried out in Georgia and the other in Alabama, illustrate the abuse that some slaves encountered at the hands of physicians. In the first, Georgia physician Thomas Hamilton conducted a series of brutal experiments on a slave to test remedies for heatstroke. The subject of these investigations, Fed, had been loaned to Hamilton as repayment for a debt owed by his owner. Hamilton forced Fed to sit naked on a stool placed on a platform in a pit that had been heated to a high temperature. Only the man's head was above ground. Over a period of 2 to 3 weeks, Hamilton placed Fed in the pit five or six times and gave him various medications to determine which enabled him best to withstand the heat. Each ordeal ended when Fed fainted and had to be revived. But note that Fed was not the only victim in this experiment; its whole purpose was to make it possible for masters to force slaves to work still longer hours on the hottest of days.
And more . . .
In the second experiment, Dr J. Marion Sims, the so-called father of modem gynecology, used three Alabama slave women to develop an operation to repair vesicovaginal fistulas. Between 1845 and 1849, the three slave women on whom Sims operated each underwent up to 30 painful operations. The physician himself described the agony associated with some of the experiments'3: "The first patient I operated on was Lucy. . . That was before the days of anaesthetics, and the poor girl, on her knees, bore the operation with great heroism and bravery." This operation was not successful, and Sims later attempted to repair the defect by placing a sponge in the bladder. This experiment, too, ended in failure. He noted:
The whole urethra and the neck of the bladder were in a high state of inflammation, which came from the foreign substance. It had to come away, and there was nothing to do but to pull it away by main force. Lucy's agony was extreme. She was much prostrated, and I thought that she was going to die; but by irrigating the parts of the bladder she recovered with great rapidity.
Sims finally did perfect his technique and ultimately repaired the fistulas. Only after his experimentation with the slave women proved successful did the physician attempt the procedure, with anesthesia, on White women volunteers.
Henrietta Lacks (born Loretta Pleasant; August 1, 1920 – October 4, 1951) was an American Black woman whose cancer cells are the source of the HeLa cell line, the first immortalized human cell line and one of the most important cell lines in medical research. An immortalized cell line reproduces indefinitely under specific conditions, and the HeLa cell line continues to be a source of invaluable medical data to the present day. Lacks was the unwitting source of these cells from a tumor biopsied during treatment for cervical cancer at Johns Hopkins Hospital in Baltimore, Maryland, U.S., in 1951. These cells were then cultured by George Otto Gey who created the cell line known as HeLa, which is still used for medical research. As was then the practice, no consent was required to culture the cells obtained from Lacks' treatment. Consistent with modern standards, neither she nor her family were compensated for their extraction or use. Even though some information about the origins of HeLa's immortalized cell lines was known to researchers after 1970, the Lacks family was not made aware of the line's existence until 1975.
About 80 percent of U.S. hospitals serve a smaller proportion of patients in racial and ethnic minority groups relative to their representation in the surrounding community, according to an analysis U.S. News & World Report released July 27 alongside its 2021-22 best hospitals rankings.
U.S. News used 2015-19 Medicare data to examine the representation of local patients who received elective care at 1,400 hospitals between 2015-19, relative to the demographics of the surrounding community.
U.S. News shared hospital-specific findings from the analysis as new healthcare equity measures on each facility's online profile. To search for a hospital, click here. The equity measures did not factor into this year's best hospitals ratings. U.S. News said it plans to add more measures in the coming years as part of its ongoing health equity initiative.
Five takeaways from the analysis:
1. Only 29 percent of hospitals treated a proportion of Black patients comparable to or higher than their community's Black population. This figure sat at 18 percent for Hispanic patients and 5 percent for Asian/Pacific Islander patients.
2. Black patients had more hospitalizations that may have been avoided with access to better preventive care compared to Medicare patients of other races.
3. A minority of hospitals served a patient population that reflected local demographics or represented a larger share of people from minority groups compared to their surrounding communities. In some cases, hospitals in the latter category were near other hospitals that disproportionately treated white patients, which suggests that community members of different races tend to receive care at different hospitals, according to U.S. News.
4. Ben Harder, managing editor and chief of health analysis at U.S. News, spoke with Becker's about the new equity ratings earlier this month and said the measures are descriptive data only — not judgments.
"We are not saying that every hospital should have exactly the same proportion of patients in their hospital as their community," he said of the analysis. "There are various reasons it might be different, and there may not be anything wrong with it, and there may not be anything possible to do about it."
5. That said, research shows patients from minority backgrounds tend to be treated at lower quality hospitals. If patients are being segregated to different hospitals or care, hospital leaders can't expect to achieve equitable outcomes, according to Mr. Harder.
"It's just descriptive, but it does paint a very informative picture about the patchwork of how different populations are cared for in this country and where they are cared for," he said. "That is critical information for us and healthcare leaders to have as we try to understand how we can address disparities in this country." To view the full analysis, click here.
Most importantly, given how the White-owned and controlled medical establishment has perpetually deceived and committed racist acts against Black people, where's the research that shows the long-term negative impact of an actual COVID-19 "cure," and not some bogusvaccine?
Therefore . . .
Given the well-documented facts (above), WHY SHOULD BLACK PEOPLE "TRUST" WHITE PEOPLE OR BRAINWASHED "UNCLE TOM" BLACK PEOPLE when it's the perpetual practice of White health care professionals and White-owned, controlled, and operated health and medical research institutions to:
(1) intentionally and repeatedly conduct unethical, unjustified, and abusive medical experiments on Black people;
(2) if hospitalized, Black patients are more likely to be denied health services and therapeutic procedures for 37 of 77 conditions (48 percent); and
(3) it's the practice of White people of power and wealth to unilaterally exploit and profit from the health of Black people and other people of color; and most importantly
(4) there are absolutely no long-term studies that validate the efficacy and the impact of negative side effects of any of the COVID-19 vaccines on Black people!
So, when YOU take an objective, factual look at the big picture of the "Black experience" in the United States of America, you find that White people of power and wealth intentionally engineered slavery, genocide, Jim Crow, segregation, redlining, high unemployment, poor education, racism, oppression, high incarceration, and have perpetually limited or prevented Black people from access to "equitable" health care. And, Black people are expected to "trust" the oppressor and get the COVID-19 vaccine, really? For the overwhelming majority of Black people, the absolute best defense against COVID-19 is to:
(a) avoid or stop being morbidly overweight or obese;
(b) avoid having low levels of Vitamin D; and
(c) avoid having underlining health conditions, such as diabetes, high blood pressure, etc.
Given the extremely high rates of obesity consistently exhibited by both Black women and Black men, it's truly pathetic that instead of actually taking concrete steps to dramatically reduce or eliminate their obesity, its the perpetual practice of morbidly overweight and obese Black people like Cedric the Entertainer, Oprah Winfrey, Gayle King, Octavia Spencer, etc., to demonstrate their ongoing failure to achieve and maintain a healthy and fit body. They should not be admired or pitied.
As validated, and published by Adela Hruby and Frank B. Hu in their research study, "The Epidemiology of Obesity: A Big Picture," if secular trends continue, by 2030 an estimated 38% of the world’s adult population will be overweight and another 20% will be obese. In the USA, the most dire projections based on earlier secular trends point to over 85% of adults being overweight or obese by 2030. Likewise, as reported by the CDC.gov, genetic changes in human populations occur too slowly to be responsible for the obesity epidemic. Nevertheless, how people respond to an environment that promotes physical inactivity and intake of high-calorie foods suggests that genes do play a role in developing obesity. Most importantly, for the overwhelming majority of people, as researched and reported by the National Institute of Health and a large body of evidence, obesity is preventable: the global epidemic of obesity has resulted mainly from societal factors that promote sedentary lifestyles and the consumption of high-fat, energy-dense diets. While genes are important in the determination of a person's susceptibility to weight gain, obesity, by and large, occurs when energy intake from what is eaten and drank exceeds energy expenditure over a protracted period. Simply put:
CALORIC
CONSUMPTION
1.
If
you burn more calories than you consume,
you will lose weight.
2.
If
you consume more calories than you burn,
you will gain weight.
3.
If
you consume calories equal to the amount
you burn, your weight will not
change.
Sadly, just like their morbidly overweight and obese White entertainment peers, such as actresses Melissa McCarthy, Chrissy Metz, Ashley Fink, Rebel Wilson, Kelly Clarkson, Kirstie Alley; and actors Billy Gardell, Louie Anderson, Jonnah Hill, James Corden, Jeff Garlin, Kevin James, etc., being rich and successful does not eliminate laziness, low self-esteem, or other emotional or psychological problems held by these . . . these "icons" of entertainment. Given the extremely high rates of obesity consistently exhibited by both Black women and Black men, these Black entertainers are not "leaders," instead, they're victims of their own overt laziness, low self-esteem or other emotional or psychological problems. Even worse, the only "leadership" they provide is to encourage Black people to take a pill for diabetes, high blood pressure, weight-reduction, etc., and to get multiple experimental vaccine shots for COVID-19 and booster shots and.
Cedric the Entertainer
IMAGES OF MORBIDLY OVERWEIGHT OR OBESE BLACK WOMEN ARE CONSTANTLY BEING PROMOTED AS ACCEPTABLE AND DESIRABLE.
Conversely, we don’t see nearly as many “promotional spots” celebrating the “beauty” of morbidly overweight and obese Black men . . . because it’s NOT beautiful, DAH!
OBSERVATION: If a man is unable to look down and see his penis, because his stomach is blocking his view, he's obese!
Just think, Oprah, Gayle King, et.c, make all that money, millions per year, but they're unable or unwilling to take concrete steps to dramatically reduce or eliminate her obesity. Meanwhile, 82.1% of all Black women over thirty-(30) years of are are morbidly overweight or obese.
Among 71,491 U.S. adults who were hospitalized with COVID-19, 27.8 percent were overweight and 50.2 were obese, according to the CDC's latest Morbidity and Mortality Weekly Report published March 8. The analysis included 148,494 patients who recieved a COVID-19 diagnosis at emergency deparments or inpatient vistits between April 1 and Dec. 31 across 238 hospitals. Of those, 71,491 were hospitalized. Those who were overweight or obese were more likely to require invasive mechanical ventilation, findings showed.
Obesity was also linked to increased risk for hospitalization and death, especially among those under age 65. As BMI rose, so did the risk, the CDC found. The risks for hospitalization, ICU admission and death were lowest among those with BMIs under 25. The "healthy weight" BMI range is between 18.5 and 24.9. The report notes that obesity is a recognized risk factor for severe COVID-19, which is possibly due to chronic inflammation that disrupts the body's immune response and impairs lung function.
"These findings highlight the clinical and public health implications of higher BMIs, including the need for intensive COVID-19 illness management as obesity severity increases, promotion of COVID-19 prevention strategies including continued vaccine prioritization and masking, and policies to ensure community access to nutrition and physical activities that promote and support a healthy BMI," the agency said.
No matter, as with most obese people, they won't live that much longer anyway.
Wait a minute . . . although atrocities against Black people are historically and typically more blatant, government-based atrocities against White people also occur; so distrust of the government is not just a "Black thing." For example, radioactive fallout from atmospheric atomic bomb tests surrounding the making of the 1956 film, "The Conqueror" in St. George, Utah continue to haunt the legacy of several iconic Hollywood actors. Several production members, including Susan Hayward, John Wayne, Agnes Moorehead, Pedro Armendáriz (who committed suicide after a diagnosis of cancer), and director Dick Powell later succumbed to cancer and cancer-related illnesses. As ascertained by People magazine in 1980, out of a cast and crew totaling 220 people, 91 of them developed some form of cancer, and 46 had died of the disease (Source: Wikipedia.com).
As of April 16, 2020 there were 28,554 deaths in the U.S. attributable to COVID-19, which increased by 715,831 for a total death count of 744,385 as of October 15, 2021, an average of 41,355 deaths per month, or 496,260 annually. Equally important if not more, about 600,000 cancer deaths happen in the U.S. each year. So, where's the zip, zap, zest, zing, and zeal to quickly create vaccines to cure or treat cancer with the same gusto as people are being "force fed" to take a quickly produced and untested vaccine for COVID-19?
The World Health Organization’s most recent figures are from 2018.
In that year, the top five causes of cancer death globally were:
The World Health Organization’s most recent figures are from 2018. In that year, the top five causes of cancer death globally were:
According to the National Cancer Institute, the list of top five causes of cancer death in the United States is similar but not the same.
Again, where's the zip, zap, zest, zing, and zeal to quickly create vaccines to cure or treat cancer, heart disease, respiratory diseases, Alzheimer's disease, and other diseases with the same gusto as people are being "force fed" to take a quickly produced and untested vaccine for COVID-19? Where?Where??Where???
Q: Well, golly gee whiz, don't "all lives matter?"
A: Obviously, not!
How do the vaccines compare?
Vaccines available in the U.S.
Vaccines Not (yet) available in the U.S.
Pfizer-BioNTech
Moderna
Johnson & Johnson
Oxford-AstraZeneca
Novavax
Pfizer-BioNTech was the first COVID-19 vaccine to receive full Food and Drug Administration (FDA) approval for people ages 16 and older in August 2021. It was also the first COVID-19 vaccine to receive FDA Emergency Use Authorization (EUA) back in December 2020, after the company reported its vaccine was highly effective at preventing symptomatic disease. This is a messenger RNA (mRNA) vaccine, which uses a relatively new technology. It must be stored in freezer-level temperatures, which can make it more difficult to distribute than some other vaccines.
Moderna’s vaccine was authorized for emergency use in the U.S. in December 2020, about a week after the Pfizer vaccine. Moderna uses the same mRNA technology as Pfizer and has a similarly high efficacy at preventing symptomatic disease. It also needs to be stored in freezer-level temperatures. In mid-August, the FDA approved a third dose of the Moderna vaccine for certain immuno-compromised individuals, including solid organ transplant recipients and those with conditions that give them an equally reduced ability to fight infections and other diseases.
The FDA granted EUA for Johnson & Johnson’s vaccine in February, 70 days after Pfizer and Moderna. Unlike the mRNA vaccines, this is a carrier, or virus vector, vaccine. It can be stored in normal refrigerator temperatures, and because it requires only a single shot, it is easier to distribute and administer.
This vaccine, which is currently being distributed in the United Kingdom and other countries, is distinguished from some of its competitors by its lower cost—it’s cheaper to make per dose, and while some of the other vaccines must be stored frozen, this one can be stored in normal refrigeration for at least six months, making it easier to distribute.
Oxford-AstraZeneca is currently studying the efficacy of a booster shoot.
This vaccine has been shown to be highly effective in clinical trials. The Novavax vaccine is a protein adjuvant. It is simpler to make than some of the other vaccines and can be stored in a refrigerator, making it easier to distribute. Novovax has studied its vaccine in combination with the influenza vaccine with positive results.
Pfizer-BioNTech
Moderna
Johnson & Johnson
Oxford-AstraZeneca
Novavax
STATUS: Approved for adults ages 16 and older in the U.S., with EUA for ages 12-15, and for specified age groups in other countries, including in the European Union (under the name Comirnaty). The CDC recommends a booster dose of the Pfizer-BioNTech vaccine for people 65 and up, residents of long-term care settings, and people 18 to 64 with underlying medical conditions or whose work may put them at higher risk of exposure to COVID-19. That latter group may include health care workers, teachers, and others. People with certain immunocompromising conditions can get a third dose of the Pfizer-BioNTech or Moderna vaccines so they can reach a level of immunity they were not able to reach after two doses. In October, Pfizer-BioNTech asked the FDA to authorize an EUA of their vaccine for children ages 5-11.
STATUS: Emergency use in the U.S and other countries, including in the European Union (it’s been approved in Switzerland) and other countries. In October, the FDA recommended a half-dose booster shot for people 65 and older, and younger adults who have medical conditions or jobs that put them at high risk. (But there are additional steps to be completed before a booster EUA is finalized).
STATUS:Emergency use in the U.S. and other countries, including in the European Union (under the name Janssen). In October, an FDA panel recommended authorization of a Johnson & Johnson booster for adults 18 and older to be given at least two months after their initial J&J shot. (But there are additional steps to be completed before a J&J booster EUA is finalized).
STATUS: Not available in the U.S., authorized for emergency use in other countries, including in the European Union (under the name Vaxzevria) and the United Kingdom.
STATUS: Not available in the U.S. at this time, but could become available in several other countries toward the end of this year and early next year.
Pfizer-BioNTech
Moderna
Johnson & Johnson
Oxford-AstraZeneca
Novavax
Recommended for: Anyone 12 or older.
Recommended for: Adults 18 and older. While the vaccine is not yet available for children, the company says its vaccine provides strong protection for children as young as 12, and it is testing its efficacy for children ages 5-11.
Recommended for: Adults 18 and older.
Recommended for: Adults 18 and older
Recommended for: The vaccine is being studied in people ages 12-84.
Pfizer-BioNTech
Moderna
Johnson & Johnson
Oxford-AstraZeneca
Novavax
Dosage: Two shots, 21 days apart; fully effective two weeks after second shot. Single-shot booster doses can be administered to those who are eligible at least six months after completion of the primary doses.
Dosage: Two shots, 28 days apart; fully effective two weeks after the second dose.
Dosage: Single shot. Fully effective two weeks after vaccination.
Dosage: Two doses, four to 12 weeks apart
Dosage: 2 doses, three weeks apart
Pfizer-BioNTech
Moderna
Johnson & Johnson
Oxford-AstraZeneca
Novavax
Common side effects: Chills, headache, pain, tiredness, and/or redness and swelling at the injection site, all of which generally resolve within a day or two of rest, hydration, and medications like acetaminophen. (If symptoms don’t resolve within 72 hours or if you have respiratory symptoms, such as cough or shortness of breath, call your doctor.) On rare occasions, the vaccine has appeared to trigger anaphylaxis, a severe reaction that is treatable with epinephrine (the drug in Epipens®). For that reason, the Centers for Disease Control and Prevention (CDC) requires vaccination sites to monitor everyone for 15 minutes after their COVID-19 shot and for 30 minutes if they have a history of severe allergies.
Common side effects: Similar to Pfizer, side effects can include chills, headache, pain, tiredness, and/or redness and swelling at the injection site, all of which generally resolve within a day or two. On rare occasions, mRNA vaccines have appeared to trigger anaphylaxis, a severe reaction that is treatable with epinephrine (the drug in Epipens®). For that reason, the CDC requires vaccination sites to monitor everyone for 15 minutes after their COVID-19 shot, and for 30 minutes if they have a history of severe allergies.
Common side effects: Fatigue, fever headache, injection site pain, or myalgia (pain in a muscle or group of muscles), all of which generally resolve within a day or two. It has had noticeably milder side effects than the Pfizer and Moderna vaccines, according to the FDA report released in late February. No one suffered an allergic reaction in clinical trials for the vaccine, according to the company.
Common side effects: Tenderness, pain, warmth, redness, itching, swelling or bruising at the injection site, all of which generally resolve within a day or two.
Rare side effects: Some countries temporarily suspended use of this vaccine in March after a small number of recipients developed blood clots and some died. In April, a European Medicines Agency (EMA) safety committee concluded "unusual blood clots with low blood platelets should be listed as very rare side effects" that could occur within two weeks of receiving the vaccine, and stressed that the benefits still outweigh the risks. In July, a study by the drugmaker, published in the Lancet, estimated the rate of thrombosis with thrombocytopenia syndrome, a clotting disorder, at 8.1 cases per million in those who received a first dose of the vaccine, and 2.3 per million after the second dose, which is comparable to incidence in the general population.
Common side effects: Injection site tenderness, fatigue, headache, muscle pain.
Pfizer-BioNTech
Moderna
Johnson & Johnson
Oxford-AstraZeneca
Novavax
FDA warnings: The FDA placed a warning label on the Pfizer vaccine regarding a “likely association” with reported cases of heart inflammation in young adults. This inflammation may occur in the heart muscle (myocarditis) or in the outer lining of the heart (pericarditis), and is considered important but uncommon—arising in about 12.6 cases per million second doses administered. The inflammation, in most cases, gets better on its own without medical intervention.
FDA warnings: The FDA placed a warning label on the Moderna vaccine regarding a “likely association” with reported cases of heart inflammation in young adults. This inflammation may occur in the heart muscle (myocarditis) or in the outer lining of the heart (pericarditis), and is considered important but uncommon—arising in about 12.6 cases per million second doses administered. The inflammation, in most cases, gets better on its own without treatment.
FDA warnings: The FDA has attached two warnings to the Johnson & Johnson vaccine. In July, the FDA attached a warning after rare cases of the neurological disorder Guillain-Barré syndrome were reported in a small number of vaccination recipients. Most of the cases occurred within 42 days after vaccination.
In April, the FDA added a warning label after ending a pause on the vaccine it had recommended “out of an abundance of caution” over an uncommon, but potentially serious, blood clotting disorder that occurred in a small number of recipients.
FDA warnings: Not available in the U.S.
FDA warnings:Not available in the U.S.
Pfizer-BioNTech
Moderna
Johnson & Johnson
Oxford-AstraZeneca
Novavax
How it works: Unlike vaccines that put a weakened or inactivated disease germ into the body, the Pfizer mRNA vaccine delivers a tiny piece of genetic code from the SARS CoV-2 virus to host cells in the body, essentially giving those cells instructions, or blueprints, for making copies of spike proteins (the spikes you see sticking out of the coronavirus in pictures online and on TV). The spikes do the work of penetrating and infecting host cells. These proteins stimulate an immune response, producing antibodies and developing memory cells that will recognize and respond if the body is infected with the actual virus.
How it works: Similar to the Pfizer vaccine, this is an mRNA vaccine that sends the body’s cells instructions for making a spike protein that will train the immune system to recognize it. The immune system will then attack the spike protein the next time it sees one (attached to the actual SARS CoV-2 virus).
How it works: This is a carrier vaccine, which uses a different approach than the mRNA vaccines to instruct human cells to make the SARS CoV-2 spike protein. Scientists engineer a harmless adenovirus (a common virus that, when not inactivated, can cause colds, bronchitis, and other illnesses) as a shell to carry genetic code on the spike proteins to the cells (similar to a Trojan Horse). The shell and the code can’t make you sick, but once the code is inside the cells, the cells produce a spike protein to train the body’s immune system, which creates antibodies and memory cells to protect against an actual SARS-CoV-2 infection.
How it works: Similar to the Johnson & Johnson vaccine, this is a carrier vaccine. Scientists engineer a harmless adenovirus as a shell to carry genetic code on the spike proteins to the cells. Once the code is inside the cells, the cells produce a spike protein to train the body’s immune system, which creates antibodies and memory cells to protect against an actual SARS-CoV-2 infection.
How it works: Unlike the mRNA and vector vaccines, this is a protein adjuvant (an adjuvant is an ingredient used to strengthen the immune response). While other vaccines trick the body’s cells into creating parts of the virus that can trigger the immune system, the Novavax vaccine takes a different approach. It contains the spike protein of the coronavirus itself, but formulated as a nanoparticle, which cannot cause disease. When the vaccine is injected, this stimulates the immune system to produce antibodies and T-cell immune responses.
Pfizer-BioNTech
Moderna
Johnson & Johnson
Oxford-AstraZeneca
Novavax
How well it works: Experts continue to learn about Pfizer’s efficacy both in the laboratory and in the real world. Pfizer’s initial Phase 3 clinical data presented in December showed its vaccine to have 95% efficacy. In April, the company announced the vaccine had 91.3% efficacy against COVID-19, based on measuring how well it prevented symptomatic COVID-19 infection seven days through up to six months after the second dose. It also found it to be 100% effective in preventing severe disease as defined by the CDC, and 95.3% effective in preventing severe disease as defined by the FDA. Another study, not yet peer-reviewed, provided more new data that brought the efficacy number down to 84% after 6 months, although efficacy against severe disease was 97%.
In August, the CDC also published studies that showed mRNA vaccine protection against infection may be waning, although the vaccines were still highly effective against hospitalization. In one CDC study, data from the state of New York showed vaccine effectiveness dropping from 91.8 to 75% against infection.
How well it works: Moderna’s initial Phase 3 clinical data in December 2020 was similar to Pfizer’s—at that point, both vaccines showed about 95% efficacy. This figure has changed over time. At six months after vaccination, the Moderna vaccine was shown to have efficacy of 90% against infection and more than 95% against developing a severe case, according to the company. In addition, while both Pfizer and Moderna still are considered highly effective, several recent studies showed Moderna to be more protective. One study published in The New England Journal of Medicine found Moderna vaccine to be 96.3% effective in preventing symptomatic illness in health care workers compared to 88.8% for Pfizer. Another, from the CDC, found Moderna’s effectiveness against hospitalization held steady over a four-month period, while Pfizer’s fell from 91% to 77%. This research is still limited and more data is needed to fully understand the differences between the two vaccines.
How well it works: 72% overall efficacy and 86% efficacy against moderate and severe disease in the U.S., according to analyses posted by the FDA in February. In early October, J&J reported in a company press release that clinical trial data showed that a booster shot given about two months after the first shot increased protection to 94% against moderate to severe disease in the U.S.
How well it works: AstraZeneca updated its data analysis of its phase 3 trials in March, showing its vaccine to be 76% effective at reducing the risk of symptomatic disease 15 days or more after receiving the two doses, and 100% against severe disease. The company also said the vaccine was 85% effective in preventing COVID-19 in people over 65.
The company’s update came a few days after the National Institute for Allergy and Infectious Diseases (NIAID) expressed concern over data AstraZeneca had submitted in advance of requesting an EUA from the FDA. The NIAID said that data may have included outdated information, which would make its efficacy data incomplete.
How well it works: 90% effective against lab-confirmed, symptomatic infection and 100% against moderate and severe disease in Phase 3 trial results released in a company statement in June. The company says the vaccine was 91% protective of people in high-risk populations such as people older than 65, those with health conditions that increase risk of complication, and those in situations where they are frequently exposed to the virus.
Pfizer-BioNTech
Moderna
Johnson & Johnson
Oxford-AstraZeneca
Novavax
THE BOTTOM LINE: Effectivesness ranges from a high of 100% to a low of 75%.
THE BOTTOM LINE: Effectivesness ranges from a high of 95% to a low of 90%.
THE BOTTOM LINE: Effectivesness ranges from a high of 94% to a low of 72%.
THE BOTTOM LINE: Effectivesness ranges from a high of 100% to a low of 76%.
THE BOTTOM LINE: Effectivesness ranges from a high of 100% to a low of 90%.
Pfizer-BioNTech
Moderna
Johnson & Johnson
Oxford-AstraZeneca
Novavax
How well it works on virus mutations: A number of studies have focused on the vaccine and the mutations. In early May, the Pfizer vaccine was found to be more than 95% effective against severe disease or death from the Alpha variant (first detected in the United Kingdom) and the Beta variant (first identified in South Africa) in two studies based on real-world vaccinations.
As far as the Delta variant, two studies reported by Public Health England that have not yet been peer reviewed showed that full vaccination after two doses is 88% effective against symptomatic disease and 96% effective against hospitalization. But Israel later reported the vaccine’s effectiveness to be 90% effective against severe disease, and 39% against infection in its population in late June and early July, based on an analysis of the country's national health statistics.
How well it works on virus mutations: Some research has suggested that Moderna’s vaccine may provide protection against the Alpha and Beta variants. In June, Moderna reported that studies showed its vaccine is effective against the Beta, Delta, Eta, and Kappa variants, although it did show it to be about two times weaker against Delta than against the original virus.
How well it works on virus mutations: Johnson & Johnson reported in July that its vaccine is also effective against the Delta variant, showing only a small drop in potency compared with its efficacy against the original strain of the virus, although one recent study suggested that the J&J vaccine is less effective against Delta. But the first study to assess the vaccine against Delta in the real world reported the vaccine to be 71% effective against hospitalization and up to 95% effective against death. The vaccine’s performance was slightly lower against the Beta variant in the study. This preliminary research was reported in August at a news conference by the Ministry of Health in South Africa. These studies have not yet been peer-reviewed or published in a scientific journal.
As of 12-16-21, the CDC no longer recommends the J&J vaccine.
For the latest update, clickhere.
How well it works on virus mutations: So far it seems to work better against the Alpha variant than the Beta variant. A paper in early February (not yet peer-reviewed) cited 74.6% efficacy against the Alpha variant. However, the vaccine did not protect as well against mild and moderate cases in people infected with the Beta variant. Therefore, South Africa halted its rollout while scientists continue to study whether the vaccine can prevent severe illness and death in people infected with this variant. As far as the Delta variant, two recent studies (neither has been peer-reviewed) showed, respectively, that full vaccination after two doses is 60% effective against symptomatic disease and 93% effective against hospitalization.
How well it works on virus mutations: Novavax says the vaccine is 93% effective against “predominantly circulating variants of concern and variants of interest.” But it’s important to note that the study was conducted in the U.S. and Mexico, when Alpha was the predominant strain in the U.S., although other variants were on the rise. More data is needed to determine the effectiveness of Novavax against the Delta variant.
Despite the established practice of typically taking approximately ten-(10) years to conduct thorough, robust research and due diligence to validate the safety and efficacy of a vaccine, nevertheless, IN LESS THAN ONE YEAR biotech and pharmaceutical companies like Moderna, Inovio, Pfizer and Merck as well as research universities like Oxford in the U.K., have all launched emergency fast-track development approaches and clinical trials to "hopefully" create a successful coronavirus vaccine. Have certain safeguards been skipped that compromise public safety, or to clandestinely manipulate the masses into a new paradigm?Hum. Yes, COVID-19 takes lives on a daily basis, but a rushed vaccine that isn’t properly tested could ultimately prove to be just as dangerous as the virus.
QUESTION 1: Given the "doubt" and "confusion" created by the lack of scientific and medical consensus on the best method to create a COVID-19 vaccine, why didn't or why hasn't the U.S. government (CDC, FDA, etc.) officially approved only one-(1) vaccine as the "standard," and then approve the mass-production of the approved vaccine via license and NDA's (non-disclosure agreements) to protect the "work product" (copyright, patent and related technologies) pertaining to the manufacture of the approved vaccine? For example, why should anyone be encouraged or required to take a vaccine (Pfizer, Johnson & Johnson, Oxford-AstraZeneca) with an effectiveness of less than 90%, when more effective vaccines (Moderna) exist?
QUESTION 2: Given the aforementioned, are you willing to let someone stick a needle in your arm and pump "whatever" into your body that might have yet-to-be-determined side-effects?
QUESTION 3: Although several vaccines exists, there's absolutely no proof the vacciness will prevent a reoccurrence; equally important, there's absolutely no proof the vaccines are protection against variant strains of the COVID-19 virus. So, are you willing to let someone stick a needle in your arm and pump "whatever" into your body that, ultimately, might not be effective?
November 11, 2021 - With a record number of new cases of Covid-19 recorded on Wednesday, the seven-day average soaring and hospitals increasingly under pressure, the health situation in Germany is rapidly worsening. This fourth wave could prove to be the worst since the beginning of the pandemic, even though some 70 percent of the adult population has been vaccinated. The scenario risks being replicated in other European countries. Advertising Germany has set a series of grim records on the health front in recent days. On November 10, the country recorded 39,676 new cases of Covid-19 in 24 hours, its highest tally during the pandemic. This despite a vaccination rate of nearly 67 percent of the adult population. The seven-day average, meanwhile, continues to reach new heights. After passing the previous record of 200 new cases per 100,000 on November 8, this closely watched index has since risen to 232.1. Source:www.france24.com
QUESTION 4: Given the collective "speed" of scientists, pharmaceutical companies, and politicians to "rush for a cure" for COVID-19, why hasn't there been a comparable rush to develop a cure for cancer and other diseases?
QUESTION 5: Eventually, after the wide dispersal of the COVID-19 vaccine throughout 2021, and dispite the existence of HIPPA and various privacy laws, will some public sector and private sector employers, schools, restaurants, stadiums, etc., posts signs to intentionally ban, to prohibit entry into private and public places, and to deny service? If so, since 78% of people who become sick and/or die from COVID-19 are morbidly overweight and obese people, where's the ban prohibiting morbidly overweight and obese people from entry into private and public places?
Hum. So, again,
the "idea" is for YOU
to take a vaccine, that's essentially untested, that'll
re-write your
genetic code, all with unknown short-term and unknown long-term impact on your overall health, and the health of your children, family, and friends - and the vaccine does not prevent you from getting COVID-19 again or from passing it on to others - you got that?
Given the published reports (at right),
it's gonna be so damn easy to say, "I told you so!"
Again, the "idea" is for YOU to take a vaccine, that's essentially untested, that'll re-write your genetic code, that may or may not require a booster shot, and may or may not provide any protection against any of the COVID-19 variants? You got that?
What's next?
BEFORE
AFTER
CLICK ABOVE IMAGE FOR VIDEO
Oh, yeah . . .
coming soon . . .
as validated by developing technology (at right), health-based discrimination
is just around the corner.
Oh, yeah . . . it's here now . . .
1. FACT: If you're fat from eating donuts and other crap, and lack of exercise, you're at greater risk for contracting COVID-19.
2. So, if you're fat, get your COVID-19 vaccine . . . and then IMMEDIATELY bring your "proof of vaccination" (POV) to the nearest Krispy Kreme and get a donut.
3. Krispy Kreme's new slogan,
"We got you fat, and
we'll keep you fat,
and that's that!"
Morbidly overweight and obese people call all the shots, make all the rules, and force you to pay more!
CLICK ABOVE IMAGE TO ENLARGE
Conversely, Atilis Gyms
(at right) has a much
better offer to the 70%
of U.S. citizens who are morbidly overweight or obese, and high risk potential victims for COVID-19 and other illnesses.
QUESTION 5: In anticipation of the next "scheduled" pandemic, what makes you think the overall character and scope of "individual rights and freedom of choice" hasn't also be pre-determined?
Something smells.
The old adage goes,
"If it sounds too good to be true, it probably is."
Vaccinated People – What We Know America’s vaccination effort is among the best in the world. However, where race is known, people of color are getting vaccinated at lower rates than white Americans. The Kaiser Family Foundation analysis reveals a signi cant disparity where race is known (about 54%) for those who have received at least one dose of vaccine as of April 13, 2021. It shows the racial/ethnic breakdown as White Americans 65%, Hispanic or Latinx 11%, Black 9%, Asian 5%, Indigenous American or Alaskan 2%, Native Hawaiian <1%, and Multiple race 9%. A YouGov poll further supports and illustrates this point as well. Among White adults polled, 26% have gotten the vaccine, compared to 17% of Black adults and 11% of Hispanic adults.
Access to Vaccines – A big part of what is occurring is disparate access to vaccination. There is a consistent pattern across states where Black and Hispanic Americans are receiving smaller shares of distributed vaccine in total. The share of vaccines going to these ethnicities is also under proportioned to the prevalence of death from COVID-19 occurring in those population segments. Additionally, due processes such as limited publication of availability in certain communities, online scheduling requirements where internet access is unavailable, or availability of vaccination only during working hours severely hinders those of lower socioeconomic status from having adequate access.
People of Color and Vaccine Hesitancy – For a myriad reasons, many members of the minority population are hesitant to receive a COVID-19 vaccine. It is unknown exactly how much this affects vaccination rates in people of color, but the phenomenon most de nitely exists. Polls early in the pandemic reported that only 40% of Black Americans would be willing to get the vaccine compared to 65% of White Americans. Fortunately, a more recent poll indicates that this number has increased to 60% for Black Americans in some areas. The issue is still pronounced due to the disparity of increased hospitalizations and deaths from COVID-19 in the African American population. This is exactly the population that you would want to have the highest rate of vaccine willingness.
To read the entire "Teamhealth.com" report, click here.
OBSERVATION 1 - DON'T BE BLACK OR NATIVE AMERICAN.
When it comes to COVID-19, you really, really don't want to be Black or Native American, because with the genocide of Native Americans, which occurred before, during, and after the enslavement of Black people, these two racial groups were intentionally bred to have poorer diets, less access to quality nutrition, diabetes, hypertension, less income, etc.
The 2020 United States Census is upon us. While the average response rate for the country as a whole is currently 60.8%, Native American tribes, such as the Navajo Nation, is under 1%. A major reason why there is such a stark contrast between response rates is because Native tribes have been especially hard hit by COVID-19. Many were not even able to receive their 2020 Census to fill out. https://www.powwows.com/hardly-any-native-tribes-are-responding-to-the-2020-census-heres-what-that-means/
Inequities exposed: COVID-19 has widened racial inequities in education, health, and the workforce. Source: Economic Policy Institute (to download PDF, click here).
OBSERVATION 2 - TESTING IS A WASTE OF TIME.
A. We're supposed to believe the United States is "at war" againist COVID-19, but such is NOT the case. As represented by the graphic of Iraq (at right), in a true "war" environment, the military acts decisively to strategically search, confine, to shutdown all ememy movements. For centuries and centuries, it's an expected practice for military operations to search from quadrant to quadrant to identify, eliminate, and eventually gain total control over opposing forces. Likewise, this is exactly what police do when they search ("sweep") a building room-by-room and subsequently shout "clear" when they validate the building is safe and secure.
Unfortunately, the "war" against COVID-19 is characterized by "open boarders," and a disingenuous testing process that, at best, is haphazard. Being "tested" has absolutely no value when you can immediately become "infected" from anyone within or outside of testing area.
For example, you're tested in Omaha, Nebraska and found to be negative. Then, you drive to a Walmart in Omaha, where you "touch" a shopping cart used by a contaminated person visiting from Bellevue, Nebraska, and now you're infected. An actual battle plan for a "war" environment would never allow soldiers to be infiltrated so easily.
If the United States truly waged a "war" against COVID-19, "Martial Law" would have been declared, and this should have happened . . . to immediately identify, isolate, treat, and eliminate COVID-19. For example:
OMAHA, NEBRASKA: Compulsory fourteen-(14) day quarantine restricting residents to their homes, and closing all city, county, state and interstate streets and highways (I-29, I-680, I-80, etc.), and closing all stores; with testing beginning in quadrant 1 through quadrant 16, with absolutely no “in and/or out” access until testing is completed. All food will be delivered to residential locations by assigned “care teams” composed of vetted health care workers, first responders (police, fire, etc.), approved volunteers, and National Guard. Then, once all testing is completed, entry into Omaha, Nebraska would only occur after entrants have been vetted (tested and cleared) and as pre-approved by authorities (local, county, state). This plan could have been extrapolated to encompass the entire state of Nebraska, thereby, strategically identifying, capturing, and eliminating contamination and spread of COVID-19, and equally important, returning people back to work within a few weeks - not months.
Yes, this plan could have been extrapolated to encompass the entire United States of America, but President Trump would have been labeled a dictator for doing so; and complaints and litigation from politicians and citizens over "States rights" would have promptly stopped this effort before it even got started.
FACTS:
1. India has a population of 1,386,197,276 which is 4.17 times larger than the United States (331,891,557);
2. As of December 14, 2020 there have been 144,130 COVID-19 deaths in India; conversely, there have been 311,073 COVID-19 deaths the United States, which is over twice as many deaths as India and counting!
We have way, way, way too many "chiefs" in the United States, which includes fifty-(50) state governors, and literally thousands and thousands of federal, state, county, and city health officials who all claim "authority" to define directed health measures to manage COVID-19. Such is the cost of "freedom."
President Trump was NOT, and is NOT the problem.
B. Does it truly make sense, is it safe to go to an area where a bunch of people (some who HAVE and some who DON’T HAVE COVID-19, which includes potential "spill-over” of COVID-19 from health care workers) who are "congested together” (in or outside of cars) to be tested for a disease that spreads via surface contact, people-to-people, and airborne? Testing does have value, but the field of contamination is pervasive and open. It would be more pragmatic and safer for health care clinicians to send residents a secure testing kit via USPS, UPS, Federal Express, etc., which we’d return.
C. There’s no actual "cure" for COVID-19, but vaccines have been developed that suggest "potential immunity." Therefore, in the absence of requiring hospitalization for ICU treatment and access to ventilators, recovery from COVID-19 typically occurs in approximately fourteen-(14) days; so why risk greater exposure to COVID-19 from a location where “haves” and “have nots” are congested for the purpose of “testing,” or creating even more confusion?
D. People of color, especially Native Americans and Black people, have always had the least access to health care, treatment, and effective management of health disparities. Plus, given my first-hand knowledge of the (quality of?) health care provided to my Dad, my Mom, and my older and younger brothers, I don’t consider it pragmatic for me to expose myself to people who’ll likely deal with me in the same fashion (mediocrity, denial of service and treatment, misdiagnosis of illness, etc.). After examinging all of the aforementioned facts above, and given "Observation 2: Testing Is A Waste of Time, #C" above, it makes more sense and it’s safer for me, and most likely everyone else, to simply self-quarantine indefinitely or for at least fourteen-(14) consecutive days (OR LONGER) from all human contact; or to at least avoid contract with Native Americans and Black people, avoid contact with people over 65 years of age, and especially, avoid contact with obese people (i.e., 4 of 5 adults!).
(The Kaiser Permanente Study) Obesity and Mortality Among Patients Diagnosed With COVID-19: Results From an Integrated Health Care Organization
Abstract Background: Obesity, race/ethnicity, and other correlated characteristics have emerged as high-profile risk factors for adverse coronavirus disease 2019 (COVID-19)–associated outcomes, yet studies have not adequately disentangled their effects.
Objective: To determine the adjusted effect of body mass index (BMI), associated comorbidities, time, neighborhood-level sociodemographic factors, and other factors on risk for death due to COVID-19.
Design: Retrospective cohort study.
Setting: Kaiser Permanente Southern California, a large integrated health care organization.
Patients: Kaiser Permanente Southern California members diagnosed with COVID-19 from 13 February to 2 May 2020.
Measurements: Multivariable Poisson regression estimated the adjusted effect of BMI and other factors on risk for death at 21 days; models were also stratified by age and sex.
Results: Among 6916 patients with COVID-19, there was a J-shaped association between BMI and risk for death, even after adjustment for obesity-related comorbidities*. Compared with patients with a BMI of 18.5 to 24 kg/m2, those with BMIs of 40 to 44 kg/m2 and greater than 45 kg/m2 had relative risks of 2.68 (95% CI, 1.43 to 5.04) and 4.18 (CI, 2.12 to 8.26), respectively. This risk was most striking among those aged 60 years or younger and men. Increased risk for death associated with Black or Latino race/ethnicity or other sociodemographic characteristics was not detected. Emerging reports suggest that obese patients who are hospitalized with COVID-19 may have worse outcomes; whether this association extends to those who are not hospitalized is unclear.
* Comorbidity - the simultaneous presence of two chronic diseases or conditions in a patient: the comorbidity of anxiety and depression in Parkinson's disease.
David A. Kass, MD, a cardiologist at John Hopkins University, elaborated on what might be behind these findings. “That the risks are higher in younger patients is probably not because obesity is particularly damaging in this age group; it is more likely that other serious comorbidities that evolve later in life take over as dominant risk factors,” he wrote. His assessment was stark: COVID-19 makes it hard to breathe, and excess fat only makes this worse.
THE OVERWHELMING MAJORITY OF COVID-19 VICTIMS (80%), THOSE HOSPITALIZED
AND THOSE WHO DIED ARE MORBIDLY OVERWEIGHT OR OBESE; THEREFORE, IF THE INTENT IS TO TRULY REDUCE OR ELIMINATE THE SPREAD OF COVID-19 . . .
BANMORBIDLY OVERWEIGHT AND OBESE PEOPLE FROM GENERAL ACCESS TO ALL PUBLIC AREAS, RESTAURANTS, PUBLIC SCHOOLS, CHURCHES, CONCERTS, ARENAS, ETC.
ALSO, BAN RESTAURANTS,
FOOD MANUFACTURERS, FAST FOOD RESTAURANTS, ETC., FROM
"SUPER-SIZING" FOOD PORTIONS.
OBSERVATION 3 - ONLY THE STRONG SURVIVE, A BUNCH OF PEOPLE ARE GOING TO DIE.
The U.S. spends more on health care as a share of the economy — nearly twice as much as the average OECD country — yet has the lowest life expectancy and highest suicide rates among the 11 nations.
The U.S. has the highest chronic disease burden and an obesity rate that is two times higher than the OECD average.
Americans had fewer physician visits than peers in most countries, which may be related to a low supply of physicians in the U.S.
Americans use some expensive technologies, such as MRIs, and specialized procedures, such as hip replacements, more often than our peers.
The U.S. outperforms its peers in terms of preventive measures — it has the one of the highest rates of breast cancer screening among women ages 50 to 69 and the second-highest rate (after the U.K.) of flu vaccinations among people age 65 and older.
Compared to peer nations, the U.S. has among the highest number of hospitalizations from preventable causes and the highest rate of avoidable deaths.
I live in a country with a blatantly inadequate supply of Personal Protective Equipment (PPE), because the manufacture of most PPEs is NOT produced in the United States - because greedy people, the majority of whom happen to be White, intentionally pay workers less to lower the cost of staffing and production, so they intentionally outsourced business production and service delivery to China, Mexico, and other nations. I live in a country were 80% of the population live paycheck-to-paycheck, and where less than 1% of the population have more wealth than over 50% of the population. I live in a country where the socio-economic status for the overwhelming majority of Black people, Latino people, and Native Americans has NEVER improved. I'm used to "managing" my life in a nation where White people make the rules (laws) and all exceptions to the rules! It's their country. White people own and/or control everything – from education to business to government; and White people unilaterally "pick and choose" if and when they'll adhere to whatever rules, laws, and contracts they establish. I'm used to "managing" my life in a country where COVID-19 provides the rich, the affluent, and the powerful (primarily White men) with a truly golden opportunity to "thin the herd."
Sadly, Black people and other people of color, and women, who've acquired education, access, and wealth are: (1) just too brainwashed and remain subservient to White people; or (2) they are just too stupid to flex the necessary business acumen to strategically improve the socio-economic status of members of their own race and/or gender. True, COVID-19 also has a dire impact on White people, but as always, the impact of COVID-19 is much worse on Black people: "when white folks catch a cold, black folks get pneumonia." In summary, as a Black man, "managing" my life during this lock down is no different than doing so at any other time; it's business as usual. I'm not being negative or apathetic; it is what it is.
OBSERVATION 4 - AN "ACT OF GOD" WILL NOT SAVE HUMANS FROM COVID-19, BECAUSE HUMANS HAVE IGNORED OR REJECTED GOD'S DIRECTIVE TO TAKE CARE OF THEIR BODIES.
I CORINTHIANS 6:19-20 (NKJV)
19 Or do you not know that your body is the temple of the Holy Spirit who is in you, whom you have from God, and you are not your own? 20 For you were bought at a price; therefore glorify God in your body and in your spirit, which are God's.
OBSERVATION 5 - MASKS DON'T WORK AND OTHER REFLECTIONS BORN OF COMMON SENSE.
If wearing a mask while you're driving alone
in your car wasn't bad enough . . .
AGAIN, COMMON SENSE QUESTION: IF MASKS DON'T IMPAIR BREATHING,
HOW COME ATHLETES DON'T WEAR MASKS WHILE COMPETING?
COMMON SENSE RESPONSE:MASKS CLEARLY IMPAIR BREATHING, AND RESTRICT
THE NATURAL EXCHANGE OF OXYGEN AND CARBON DIOXIDE.
(Below) Eddie Griffin asks,
"If a mask can't stop the smell of gas from yo' ass,
how's a mask going to save yo ass?"
CAN YOU TRUST DOCTORS? ABSOLUTELY NOT!"
"Incestuous" Self-Serving Medical boards often protect doctors over patients, CBS News finds
And if you can't "trust" the doctors, how can you possibly trust the science?
WHAT'S THE SINGLE MOST IMPORTANT DRIVING FACTOR FOR FOR-PROFIT AND NON-PROFIT HEALTHCARE PROVIDERS? IT'S NOT HEALTH, IT'S MONEY. COVID-19 IS ABSOLUTELY GREAT FOR BUSINESS!
HCA's profit more than triples to $2.3B in Q3
Alia Paavola - Friday, October 22nd, 2021
Nashville, Tenn.-based HCA Healthcare saw strong growth in revenue and profit in the third quarter of 2021 compared to the same period last year.
The 183-hospital system posted revenue of $15.3 billion in the quarter ended Sept. 30, up 14.8 percent from the $13.3 billion recorded in the third quarter of 2020.
Compared to the third quarter of 2020, HCA said same-facility admissions increased 6.8 percent; emergency room visits increased 31.2 percent; inpatient surgeries declined 4.9 percent; and same-facility outpatient surgeries increased 6.4 percent.
Revenue per equivalent admission increased 5.2 percent because of increases in the acuity of patients and favorable payer mix, HCA said. After factoring in expenses and nonoperating items, HCA's net income totaled $2.3 billion in the third quarter of 2021, more than triple the $688 million recorded in the third quarter last year.
HCA said the results of the third quarter include more than $1 billion in gains on the sale of four hospitals in Georgia and other money from investments.
For the nine months ending Sept. 30, HCA recorded a net income of $5.1 billion on $43.6 billion in revenue. In the same nine-month period in 2020, HCA saw a net income of $2.3 billion on $37.2 billion in revenue.
"During the third quarter we experienced the most intense surge yet of the pandemic, and our colleagues and physicians delivered record levels of patient care to meet the demand caused by the delta variant," said Sam Hazen, CEO of HCA Healthcare. "Once again, the disciplined operating culture and strong execution by our teams were on display. I want to thank them for their tremendous work and dedication to serving others."
Tenet's operating income hits $1B in Q3
Alia Paavola - Wednesday, October 20th, 202
Dallas-based Tenet Healthcare saw many of its key financial metrics improve in the third quarter of 2021, according to its financial report released Oct. 20.
In the third quarter ending Sept. 30, the for-profit hospital system saw its net operating revenue hit $4.9 billion, up 7.4 percent from the $4.6 billion recorded in the same period last year.
Tenet saw revenue growth in its hospital and ambulatory divisions. In its hospital segment, revenue for the third quarter grew 6 percent year over year to $4 billion. Tenet attributed the growth to higher volumes and higher patient acuity. It said hospital segment growth was partially offset, given the Aug. 1 sale of five of its Florida hospitals. Tenet's ambulatory segment recorded $666 million in revenue in the third quarter, an increase of 17.9 percent compared to the same period last year.
Tenet did see revenue declines in its revenue cycle division, Conifer. Tenet said the revenue decline was primarily due to previously disclosed contract changes
The for-profit health system saw its operating expenses increase in the third quarter year over year, driven by a 5.5 percent increase in supply costs and a 3.1 percent increase in salary, wages and benefit costs.
Tenet ended the third quarter with an operating income of $1 billion. In comparison, in the same quarter last year, Tenet had an operating income of $271 million.
After factoring in nonoperating items, including interest expenses, debt repayment and income tax expense, Tenet ended the period with a net income of continuing operations available to common shareholders of $448 million. Last year, Tenet recorded a net loss of $197 million.
"We are very pleased with our performance during the quarter and the drive to deliver consistent and sustainable growth across each of our operating segments," said Ron Rittenmeyer, executive chair of Tenet. "With the ongoing implementation of our transformation, we are positioning Tenet for continued high margin growth and strong cash flow generation."
During the third quarter, Tenet completed the sale of five of its hospitals for $1.1 billion. It used the proceeds from the deal to repay outstanding debt, which reduced future annual cash interest payments by about $50 million.
Health care executives have amassed huge deferred compensation accounts, buoyed by taxpayer investments
The CEO of Centene, the nation’s largest Medicaid provider, had the second-largest “top hat” plan in the S&P 500 in 2022, valued at $328 million.
Fueled by COVID-19 vaccine profits, Pfizer CEO Albert Bourla enjoyed a 37 percent increase in the value of his deferred compensation account over the past year, from $29.5 million to $44.4 million at the end of 2022.
Joe Rogan exposes Sanjay Gupta and CNN's propaganda
Second opinion? Do NOT consult YouTube.com
Prior to having surgery, it's a well-established and respected practice for patients to conduct their own "due diligence," including getting a "second opinion" from a variety of medical and scientific subject matter experts.
However, despite the fact Dr. Anthony Fauci, the CDC, and the World Health Organization have frequently flip-flopped on treatment strategies for COVID-19, including vaccines, wearing masks, and social distancing, nevertheless, YouTube.com does not allow any kind of legitimate, professional dissent, even from subject matter experts, doctors, and scientists who hold as much if not more expertise than their peers at the CDC and WHO. It's clearly the hypocrisy of YouTube.com to allow "subject matter experts" to post videos with "differing opinions" on car repair, computer repair, and even health, fitness, and nutrition, but people are prohibited from posting "differing opinions" on how to make an informed personal decision on COVID-19.
YouTube.com COVID-19 medical misinformation policy
The safety of our creators, viewers, and partners is our highest priority. We look to each of you to help us protect this unique and vibrant community. It’s important you understand our Community Guidelines, and the role they play in our shared responsibility to keep YouTube safe. Take the time to carefully read the policy below. You can also check out this page for a full list of our guidelines.
YouTube doesn't allow content about COVID-19 that poses a serious risk of egregious harm.
YouTube doesn't allow content that spreads medical misinformation that contradicts local health authorities’ (LHA) or the World Health Organization’s (WHO) medical information about COVID-19. This is limited to content that contradicts WHO or local health authorities’ guidance on:
Treatment Prevention Diagnosis Transmission Social distancing and self isolation guidelines The existence of COVID-19
Note: YouTube’s policies on COVID-19 are subject to change in response to changes to global or local health authorities’ guidance on the virus. There may be a delay between new LHA/WHO guidance and policy updates given the frequency with which this guidance changes, and our policies may not cover all LHA/WHO guidance related to COVID-19.
Our COVID-19 policies were first published on May 20, 2020.
What this policy means for you
If you're posting content
Don’t post content on YouTube if it includes any of the following:
Treatment misinformation:
Content that encourages the use of home remedies, prayer, or rituals in place of medical treatment such as consulting a doctor or going to the hospital Content that claims that there’s a guaranteed cure for COVID-19 Content that recommends use of Ivermectin or Hydroxychloroquine for the treatment of COVID-19 Claims that Hydroxychloroquine is an effective treatment for COVID-19 Categorical claims that Ivermectin is an effective treatment for COVID-19 Claims that Ivermectin and Hydroxychloroquine are safe to use in the treatment COVID-19 Other content that discourages people from consulting a medical professional or seeking medical advice
Prevention misinformation:
Content that promotes prevention methods that contradict local health authorities or WHO.
Claims that there is a guaranteed prevention method for COVID-19 Claims that any medication or vaccination is a guaranteed prevention method for COVID-19 Content that recommends use of Ivermectin or Hydroxychloroquine for the prevention of COVID-19 Claims that Ivermectin and Hydroxychloroquine are safe to use in the treatment COVID-19 Claims that wearing a mask is dangerous or causes negative physical health effects Claims that masks do not play a role in preventing the contraction or transmission of COVID-19 Claims about COVID-19 vaccinations that contradict expert consensus from local health authorities or WHO Claims that an approved COVID-19 vaccine will cause death, infertility, miscarriage, autism, or contraction of other infectious diseases Claims that an approved COVID-19 vaccine will contain substances that are not on the vaccine ingredient list, such as biological matter from fetuses (e.g. fetal tissue, fetal cell lines) or animal products Claims that an approved COVID-19 vaccine will contain substances or devices meant to track or identify those who’ve received it Claims that COVID-19 vaccines will make people who receive them magnetic Claims that an approved COVID-19 vaccine will alter a person’s genetic makeup Claims that COVID-19 vaccines do not reduce risk of contracting COVID-19 Claims that any vaccine causes contraction of COVID-19 Claims that a specific population will be required (by any entity except for a government) to take part in vaccine trials or receive the vaccine first Content that promotes the use of unapproved or homemade COVID-19 vaccines
Instructions to counterfeit vaccine certificates, or offers of sale for such documents
Diagnostic misinformation: Content that promotes diagnostic methods that contradict local health authorities or WHO.
Claims that approved COVID-19 tests are dangerous or cause negative physical health effects Claims that approved COVID-19 tests cannot diagnose COVID-19
Transmission misinformation: Content that promotes transmission information that contradicts local health authorities or WHO. Content that claims that COVID-19 is not caused by a viral infection Content that claims COVID-19 is not contagious Content that claims that COVID-19 cannot spread in certain climates or geographies Content that claims that any group or individual has immunity to the virus or cannot transmit the virus
Social distancing and self isolation misinformation: Content that disputes the efficacy of local health authorities’ or WHO's guidance on physical distancing or self-isolation measures to reduce transmission of COVID-19.
Content that denies the existence of COVID-19:
Denial that COVID-19 exists Claims that people have not died or gotten sick from COVID-19 Claims that the virus no longer exists or that the pandemic is over Claims that the symptoms, death rates, or contagiousness of COVID-19 are less severe or equally as severe as the common cold or seasonal flu Claims that the symptoms of COVID-19 are never severe
This policy applies to videos, video descriptions, comments, live streams, and any other YouTube product or feature. Keep in mind that this isn't a complete list. Please note these policies also apply to external links in your content. This can include clickable URLs, verbally directing users to other sites in video, as well as other forms.
Examples
Here are some examples of content that’s not allowed on YouTube:
Denial that COVID-19 exists Claims that people have not died from COVID-19 Claims that any vaccine is a guaranteed prevention method for COVID-19 Claims that a specific treatment or medicine is a guaranteed cure for COVID-19 Claims that hydroxychloroquine saves people from COVID-19 Promotion of MMS (Miracle Mineral Solution) for the treatment of COVID-19 Claims that certain people have immunity to COVID-19 due to their race or nationality Encouraging taking home remedies instead of getting medical treatment when sick Discouraging people from consulting a medical professional if they’re sick Content that claims that holding your breath can be used as a diagnostic test for COVID-19 Videos alleging that if you avoid Asian food, you won’t get the coronavirus Videos alleging that setting off fireworks can clean the air of the virus and will prevent the spread of the virus Claims that COVID-19 is caused by radiation from 5G networks Videos alleging that the COVID-19 test is the cause of the virus Claims that countries with hot climates will not experience the spread of the virus Videos alleging that social distancing and self-isolation are not effective in reducing the spread of the virus Claims that wearing a mask causes oxygen levels to drop to dangerous levels Claims that masks cause lung cancer or brain damage Claims that wearing a mask gives you COVID-19 Claims that the COVID-19 vaccine will kill people who receive it Claims that the COVID-19 vaccine will be used as a means of population reduction Videos claiming that the COVID-19 vaccine will contain fetal tissue Claims that the flu vaccine causes contraction of COVID-19 Claims that COVID-19 vaccines are not effective in preventing the spread of COVID-19 Claims that the COVID-19 vaccine causes contraction of other infectious diseases or makes people more vulnerable to contraction of other infectious diseases Claims that the COVID-19 vaccines contain a microchip or tracking device Claims that achieving herd immunity through natural infection is safer than vaccinating the population Claims that COVID-19 never causes serious symptoms or hospitalization Claims that the death rate from the seasonal flu is higher than the death rate of COVID-19 Claims that people are immune to the virus based on their race Claims that children cannot or do not contract COVID-19 Claims that there have not been cases or deaths in countries where cases or deaths have been confirmed by local health authorities or the WHO
Educational, documentary, scientific or artistic content
We may allow content that violates the misinformation policies noted on this page if that content includes additional context in the video, audio, title, or description. This is not a free pass to promote misinformation. Additional context may include countervailing views from local health authorities or medical experts. We may also make exceptions if the purpose of the content is to condemn, dispute, or satirize misinformation that violates our policies. We may also make exceptions for content showing an open public forum, like a protest or public hearing, provided the content does not aim to promote misinformation that violates our policies.
What happens if content violates this policy
If your content violates this policy, we’ll remove the content and send you an email to let you know. If this is your first time violating our Community Guidelines, you’ll likely get a warning with no penalty to your channel. If it’s not, we may issue a strike against your channel. If you get 3 strikes within 90 days, your channel will be terminated. You can learn more about our strikes system here.
We may terminate your channel or account for repeated violations of the Community Guidelines or Terms of Service. We may also terminate your channel or account after a single case of severe abuse, or when the channel is dedicated to a policy violation. You can learn more about channel or account terminations here.
WHAT ABOUT YOUR CONSTITUTIONAL RIGHT OF "FREEDOM" AND "PRIVACY" AND YOUR RIGHT TO "PROTEST" AND MORE?"
As it turns out, far too many power brokers in your local, state, and federal government don't care about your constitutional right of "freedom" and "privacy" and your right to "protest." Instead of focusing on viable solutions, it remains the demonstrated practice for politicians, health care professionals, and the news media to ONLY "promote and champion" the negative; and to criticize and ridicule all dissension. It's their collective mandate for people to cower and submit to their rule, to relinquish their intellectual and physical freedoms; and most importantly, to acquiesce their income to helplessness, poverty and homelessness. Fortunately, some people openly disagree.
Remember, it's coming . . . an I.D. for this, an I.D. for that . . .
Glenn Thomas Jacobs (born April 26, 1967) is an American politician, actor, and professional wrestler (7' tall, 343 pounds), currently signed to WWE, where he works under the ring name Kane. As a Republican, he is the Mayor of Knox County, Tennessee since 2018. Mayor Jacobs' letter to President Biden is presented below.
Mike Rowe was sitting in an airport, perhaps bored, as one might be in the same situation. So, Rowe went to Facebook, and with nothing more than "common sense," on September 16, 2021 he posted the following assessment of President Biden's latest COVID-19 vaccine commandment.
"Last week, as I'm sure you're aware, moments after assuring the country that the vaccines he and millions of others have taken are "incredibly effective," President Biden said, "We must now protect the vaccinated workers from the unvaccinated workers." You don't have to be a scientist to hear a message like that and pose a couple of very reasonable queries.
1) If the vaccines are effective, why do the vaccinated need to be protected from the unvaccinated? And
2) If the vaccines are not effective, then why should the unvaccinated get one?
Our fully vaccinated President still supports a travel ban that keeps my vaccinated friends overseas from reentering the country. Why? He still wears a mask in public – even when he's outdoors. Why? Last week, President Biden could have congratulated all vaccinated Americans for getting back to living their lives without fear. Instead, he got angry. He literally accused the unvaccinated of "standing in the way of protecting the large majority of Americans who have done their part and want to get back to life as normal." In short, Joe Biden doesn't appear to be living his life any differently than he did before getting vaccinated."
Entrepreneur Perfectly Explains What the Canadian
Truckers "Freedom Convoy" Blockade Is All About
A Parent Perfectly Explains, "Why parents are mad?"
"Identity politics" is more important to some elected officials than
allowing the communication of actual "facts" about COVID-19!
QUESTION 1: Do you realize how many people did not have to die, how many lives could have been saved, if the rich, the affluent, and the powerful had acted responsibly and humanely in managing all aspects of COVID-19, PPEs, vaccines, etc.?
QUESTION 2: As detailed above, given the Good, the Bad, and the Very Ugly, and the perpetual failure and refusal of key decision makers (the rich, the affluent, and the powerful) to act "humanely" for the greater benefit of all U.S. citizens, is there any chance the U.S. might effectively and humanely prepare for or perhaps avoid the next pandemic?
QUESTION 3: Do you really think "things" will get back to normal when the threat of COVID-19 has been dramatically reduced or eliminated?Really? Read this.
RECOMMENDATION:
It doesn't really matter.
Put a stop to the social distancing. Re-open all businesses, restaurants, and schools. Give people the option to wear a mask or not. Re-open and fill all of the high school, college, and professional football, basketball, and concert venues. Yes, some people will likely die, especially Native Americans, Black people, and a lot of obese people; and yes, only the strong survive. Life's not fair. That's life! IT'S TIME TO THIN THE HERD.
People with the greatest risk for becoming a victim of COVID-19 are the four-(4) of five-(5) adults who are morbidly overweight or obese, especially Black people. Consequently, with more death and illiness, hopefully, health and wellness will finally become a true "growth industry." If you're fat, obese, with an underlying health condition, and/or over sixty-five-(65) years of age then you're at greatest risk, and you need to act with a heightened level of common sense. Yes, some but not all hospitals will become overburden, but so what. Hospitals are NOT in businesss to provide "health care," on the contrary, hospitals are in business to make money, to make a profit (or "revenue" if operating as a so-called non-profit) by providing a medical service. Hospitals will hire more staff, expand existing facilities or build new facilities, which will spur job growth and economic development. Likewise, death will also become a growth industry with cemeteries, memorial parks, churches, and pastors conducting thousands and thousands of funerals. Welcome to the challenges and joys of a free and open capitalist society. Am I serious? Yes, I am. So let's re-open, because as represented by the blatantly accurate sarcasm in the video below, the constant lack of consistency in managing COVID-19 validates it really doesn't matter what you do.
If you're still confused, uncertain if you should get the vaccine, Abbott and Costello can clarify everything.
ABBOTT AND COSTELLO’S
‘WHO’S BEEN VACCINATED??
‘You can’t come in here!’
‘Why not?’
‘Well because you’re unvaccinated.’
But I’m not sick.’
‘It doesn’t matter.’
‘Well, why does that guy get to go in?’
‘Because he’s vaccinated.’
‘But he’s sick!’
‘It’s alright. Everyone in here is vaccinated.’
‘Wait a minute. Are you saying everyone in there is vaccinated?’
‘Yes.’
‘So then why can’t I go in there if everyone is vaccinated?’
‘Because you’ll make them sick.’
‘How will I make them sick if I’m NOT sick and they’re vaccinated.’
‘Because you’re unvaccinated.’
But they’re vaccinated.’
‘But they can still get sick.’
‘So what the heck does the vaccine do?’
‘It vaccinates.’
‘So vaccinated people can’t spread covid?’
‘Oh no. They can spread covid just as easily as an unvaccinated person.’
‘I don’t even know what I’m saying anymore. Look. I’m not sick.
‘Ok.’
‘And the guy you let in IS sick.’
‘That’s right.’
And everybody in there can still get sick even though they’re vaccinated.’
‘Certainly.’
‘So why can’t I go in again?’
‘Because you’re unvaccinated.’
‘I’m not asking who’s vaccinated or not!’
‘I’m just telling you how it is.’
‘Nevermind. I’ll just put on my mask.’
‘That’s fine.’
‘Now I can go in?’
‘Absolutely not?’
‘But I have a mask!’
‘Doesn’t matter.’
I was able to come in here yesterday with a mask.’
‘I know.’
So why can’t I come in here today with a mask? ….If you say ‘because I’m unvaccinated’ again, I’ll break your arm.’
‘Take it easy buddy.’
‘So the mask is no good anymore.’
‘No, it’s still good.’
‘But I can’t come in?’
‘Correct.’
‘Why not?’
‘Because you’re unvaccinated.’
But the mask prevents the germs from getting out.’
‘Yes, but people can still catch your germs.’
But they’re all vaccinated.’
‘Yes, but they can still get sick.’
‘But I’m not sick!!’
‘You can still get them sick.’
‘So then masks don’t work!’
‘Masks work quite well.’
‘So how in the heck can I get vaccinated people sick if I’m not sick and masks work?’
‘Third base.’
End Scene.
Abbott & Costello and their legendary skit, "Who's on first?"
Researcher: ‘We Made a Big Mistake’ on COVID-19 Vaccine.
by Joseph Mercola - May 16, 2022 - The Epoch Times
Canadian immunologist and vaccine researcher Byram Bridle, Ph.D., has gained access to Pfizer’s biodistribution study from the Japanese regulatory agency. The research demonstrates a huge problem with all COVID-19 vaccines
The assumption that vaccine developers have been working with is that the mRNA in the vaccines would primarily remain in and around the vaccination site. Pfizer’s data, however, show the mRNA and subsequent spike protein are widely distributed in the body within hours.
This is a serious problem, as the spike protein is a toxin shown to cause cardiovascular and neurological damage. It also has reproductive toxicity, and Pfizer’s biodistribution data show it accumulates in women’s ovaries.
Once in your blood circulation, the spike protein binds to platelet receptors and the cells that line your blood vessels. When that happens, it can cause platelets to clump together, resulting in blood clots, and/or cause abnormal bleeding.
Pfizer documents submitted to the European Medicines Agency also show the company failed to follow industry-standard quality management practices during preclinical toxicology studies and that key studies did not meet good laboratory practice standards.
The more we learn about the COVID-19 vaccines, the worse they look. In a recent interview with Alex Pierson, Canadian immunologist and vaccine researcher Byram Bridle, Ph.D., dropped a shocking truth bomb that immediately went viral, despite being censored by Google.
To download this entire article, please click here.
First Amendment to the United States Constitution - Congress shall make no law respecting an establishment of religion, or prohibiting the free exercise thereof; or abridging the freedom of speech, or of the press; or the right of the people peaceably to assemble, and to petition the Government for a redress of grievances.
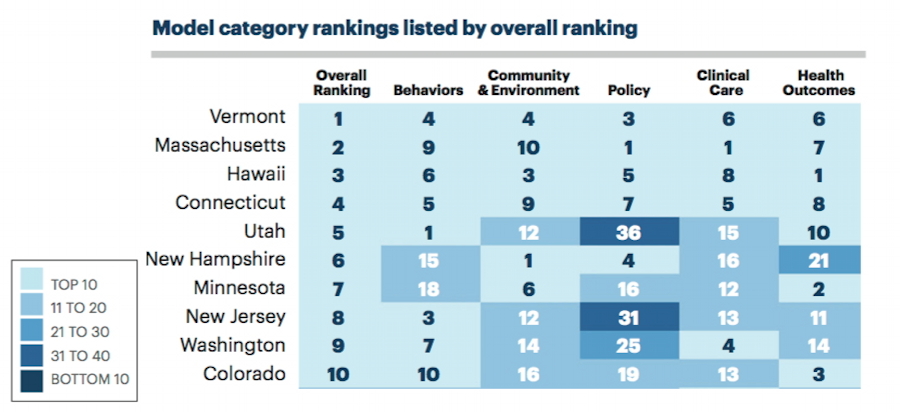
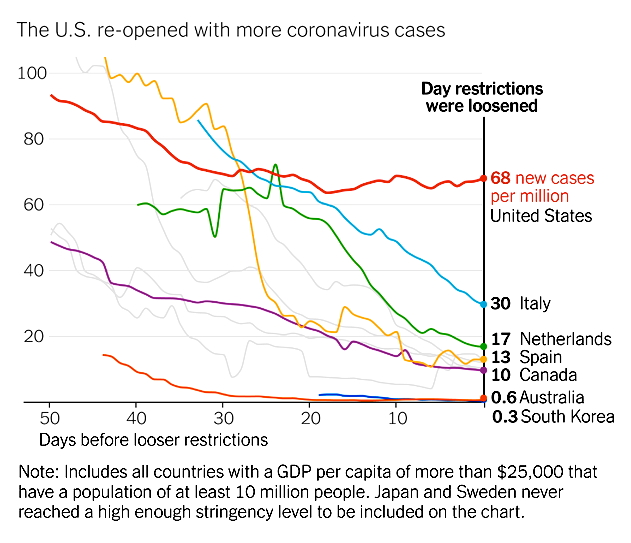


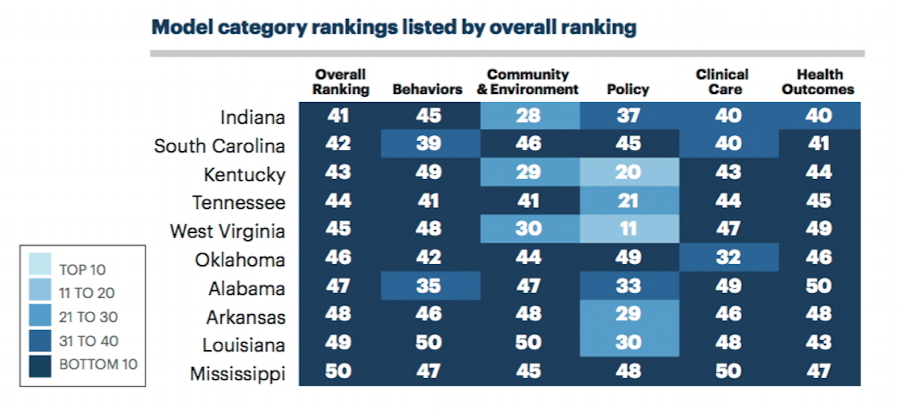
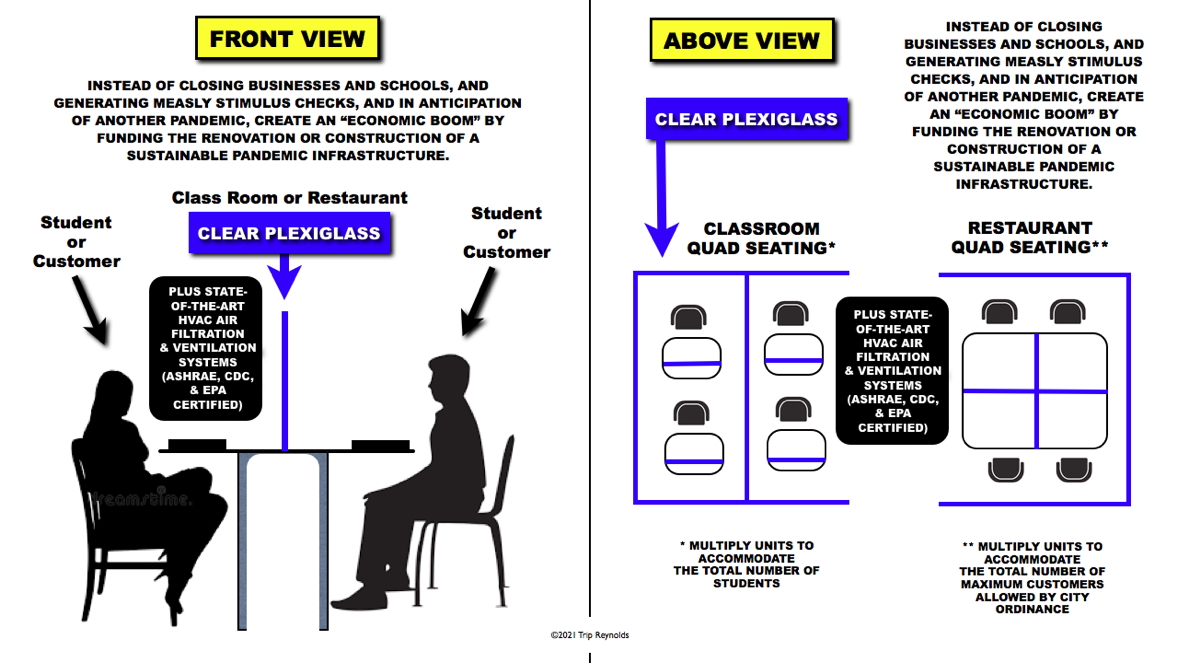
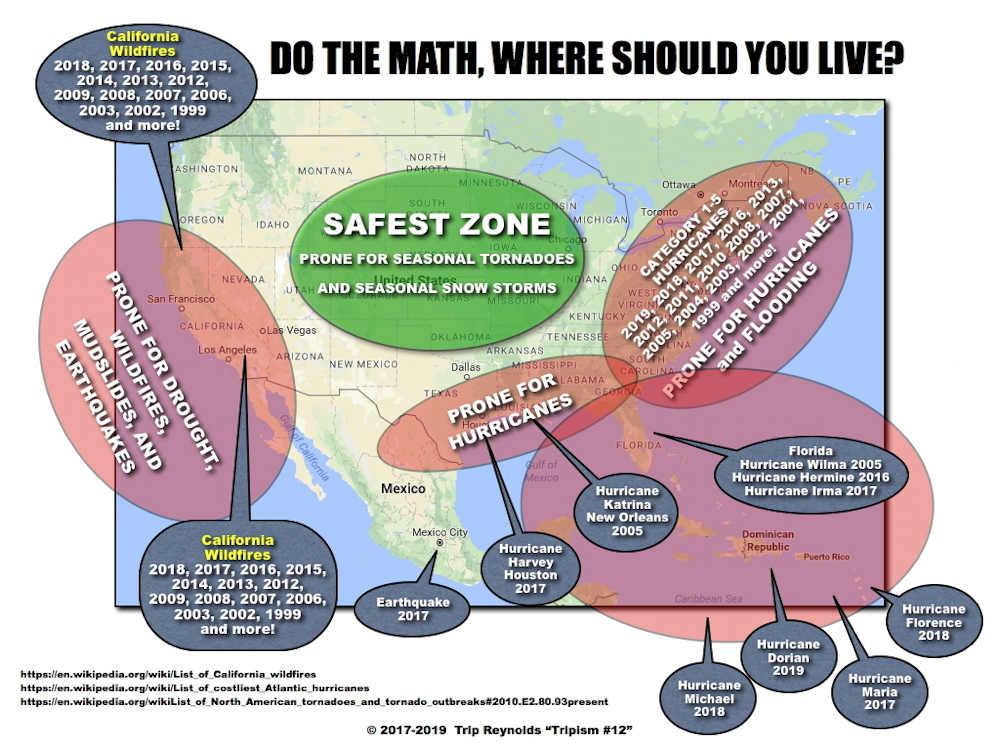






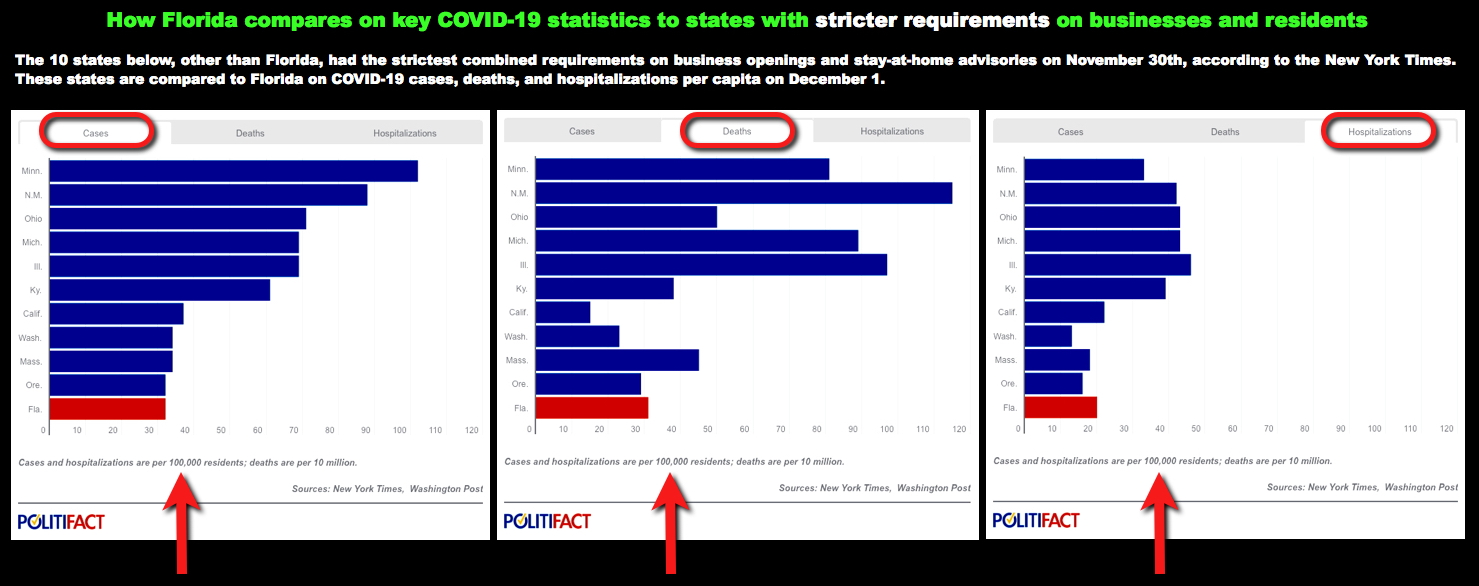
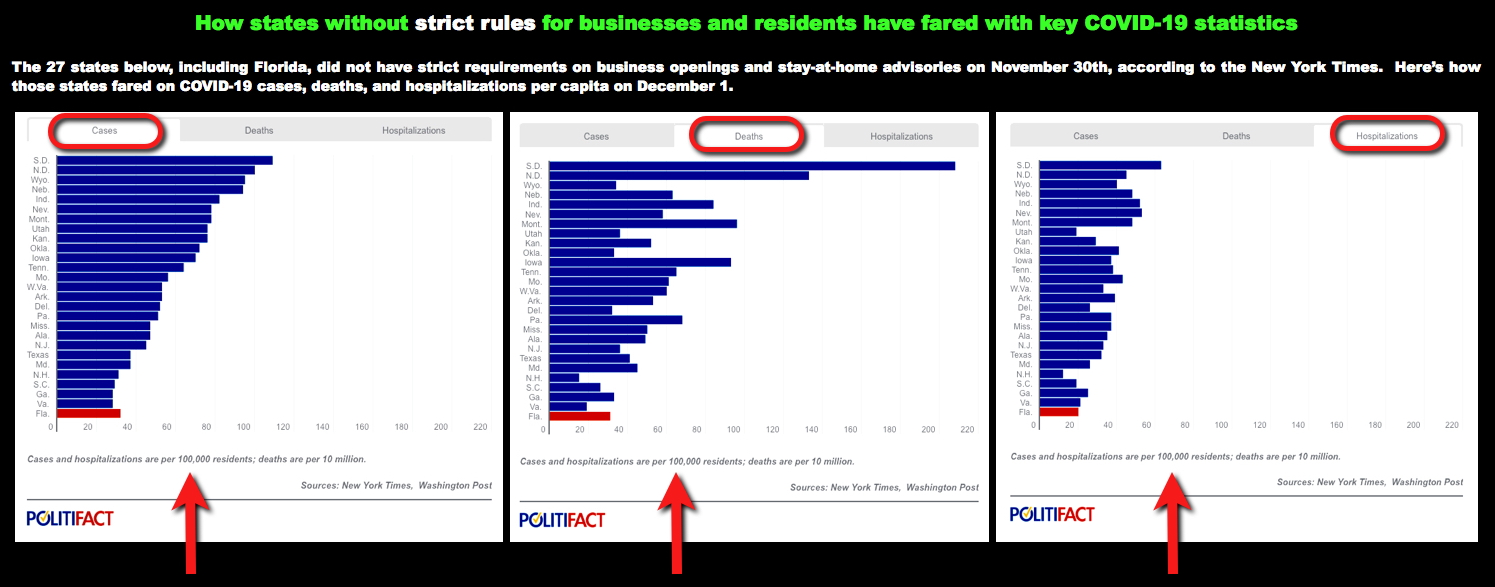
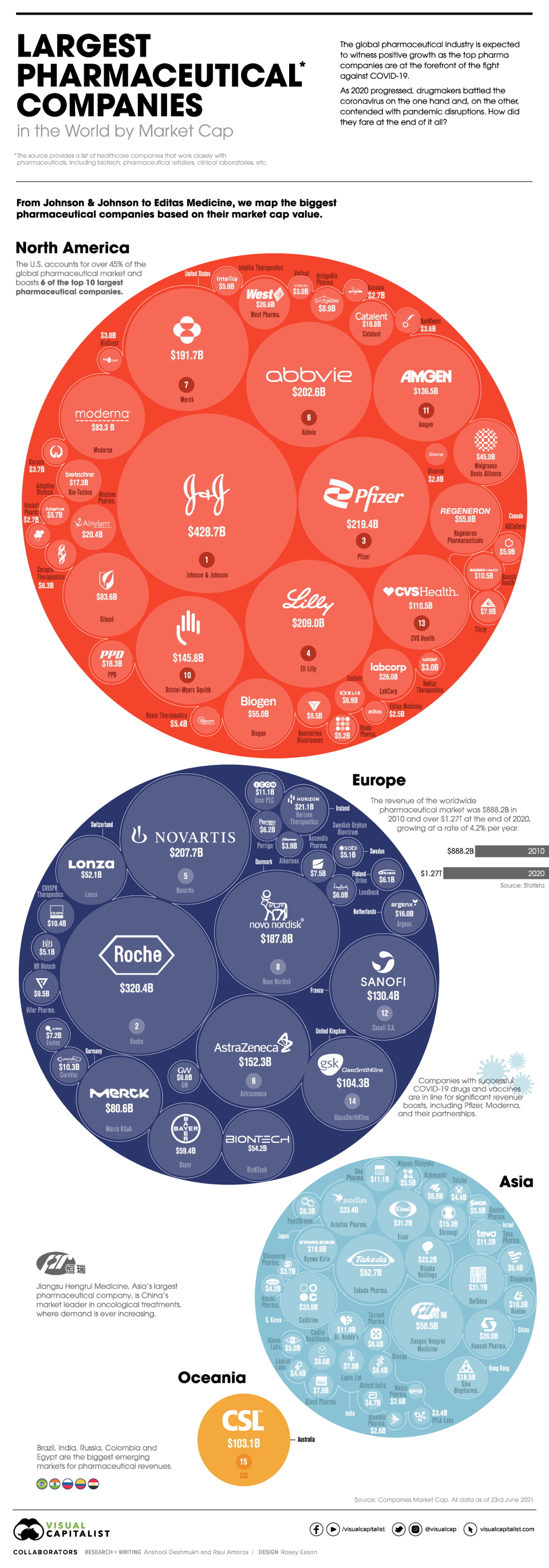
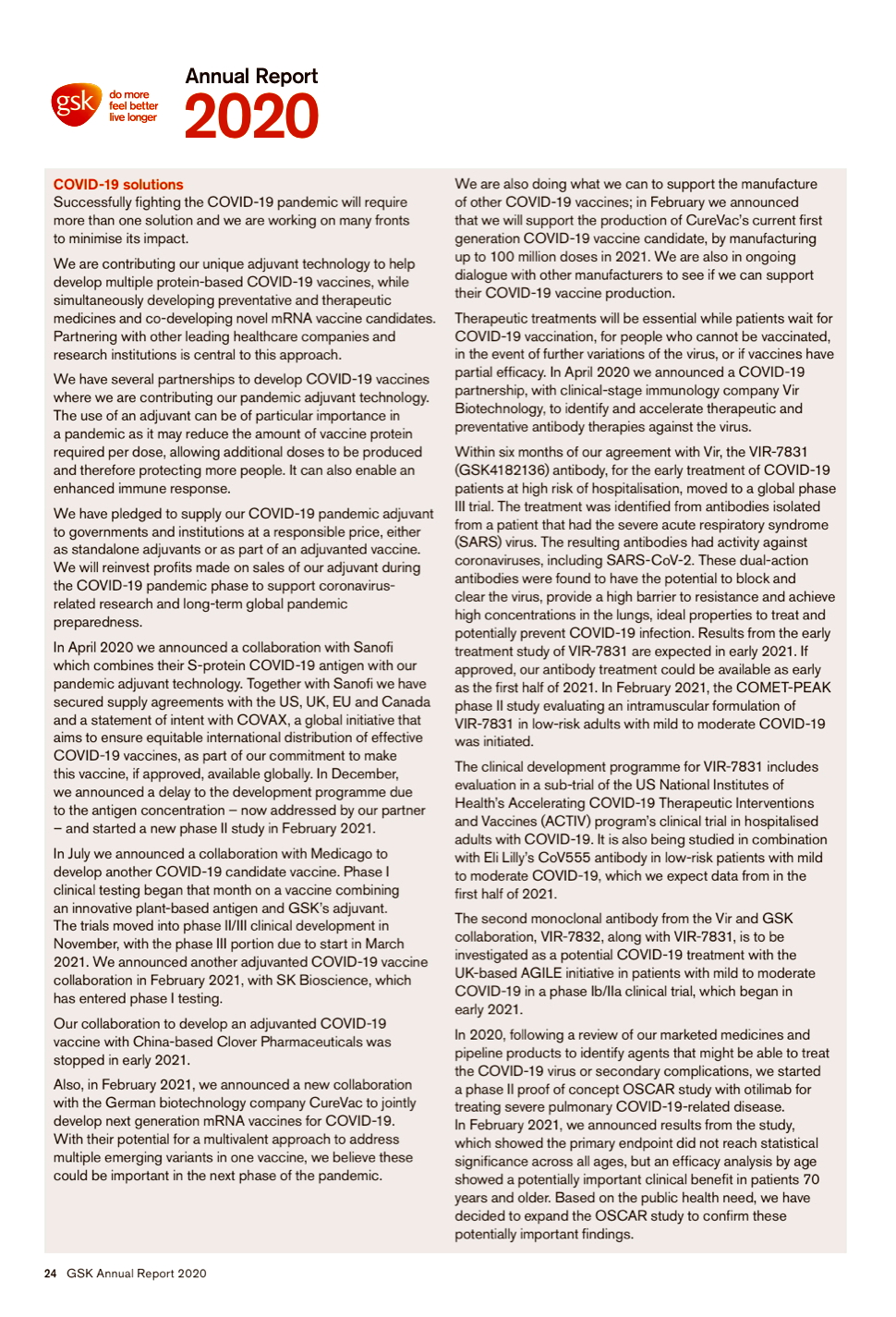
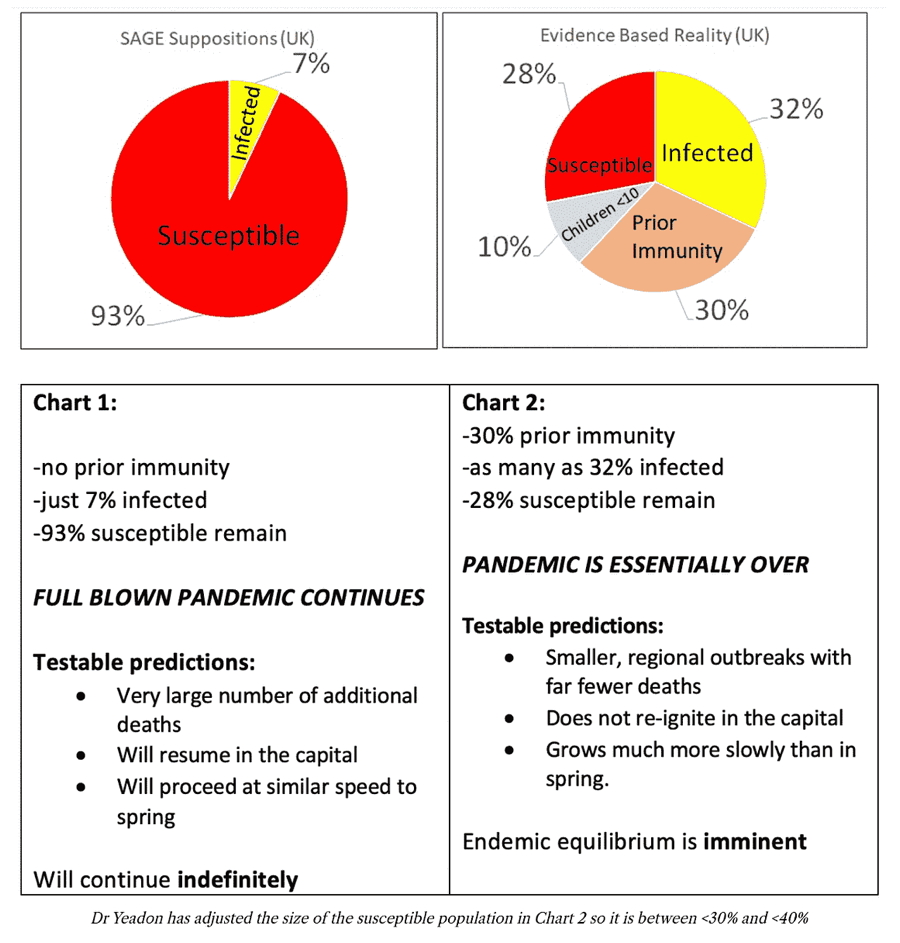

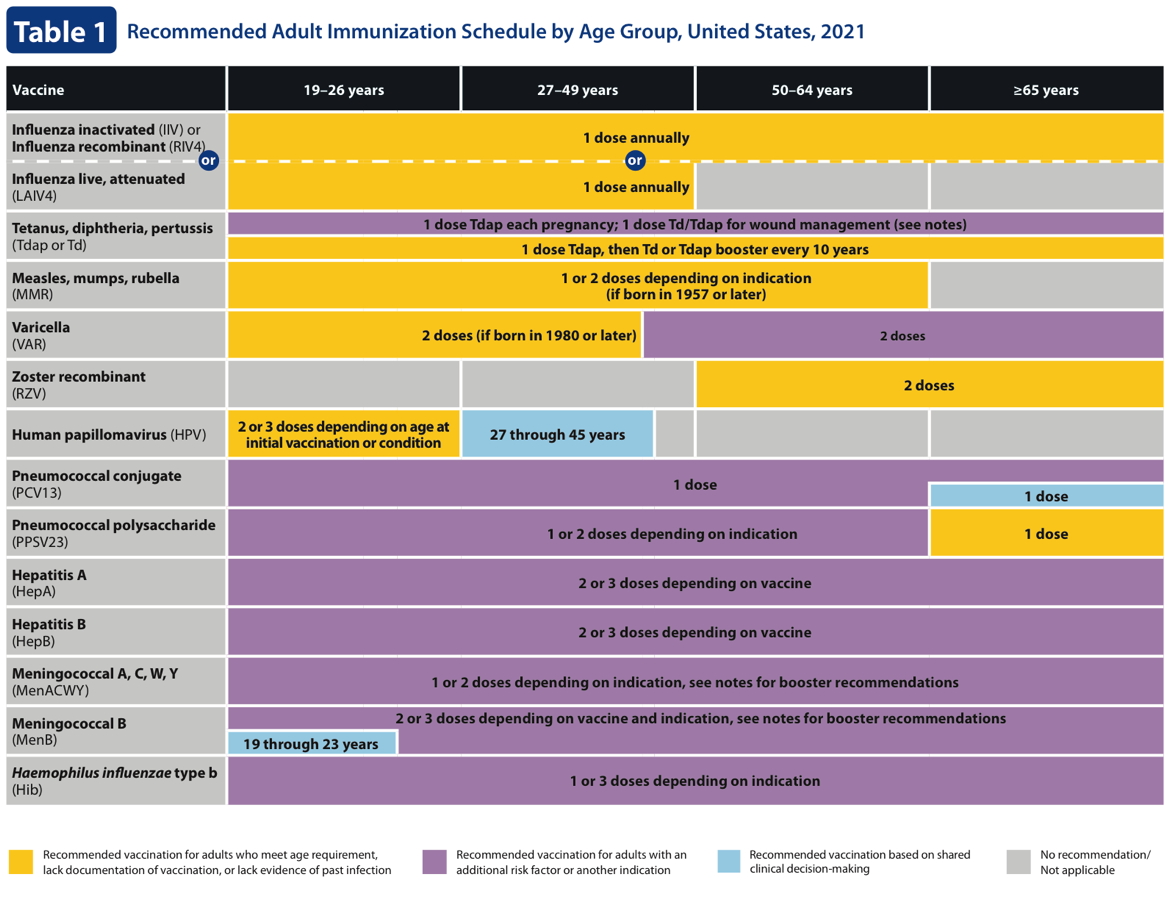
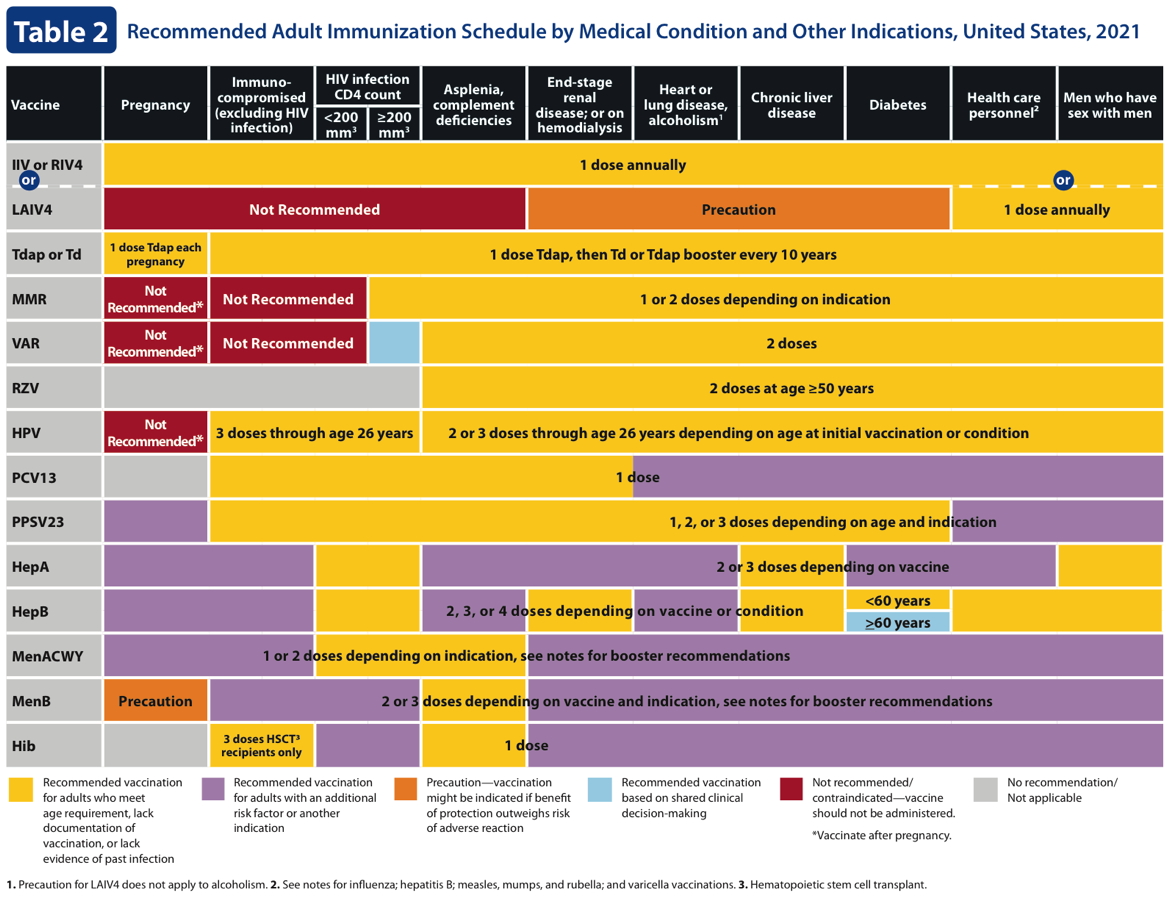








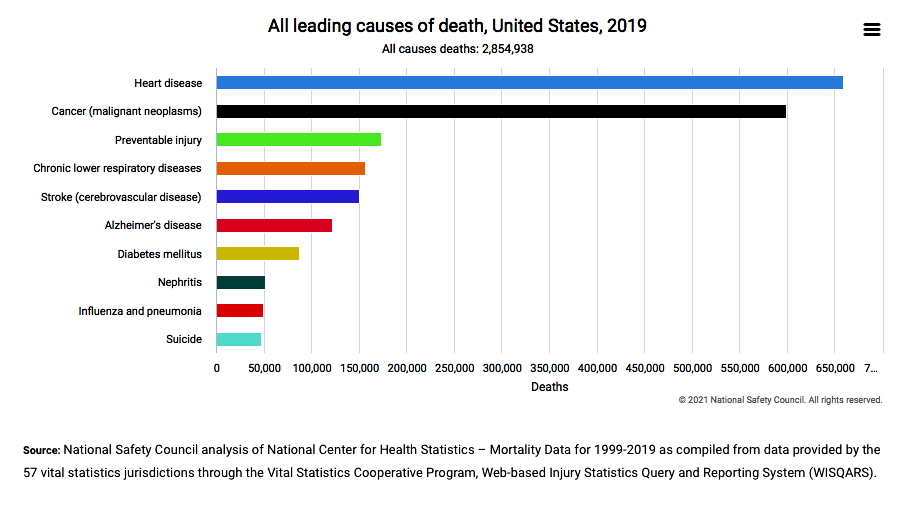
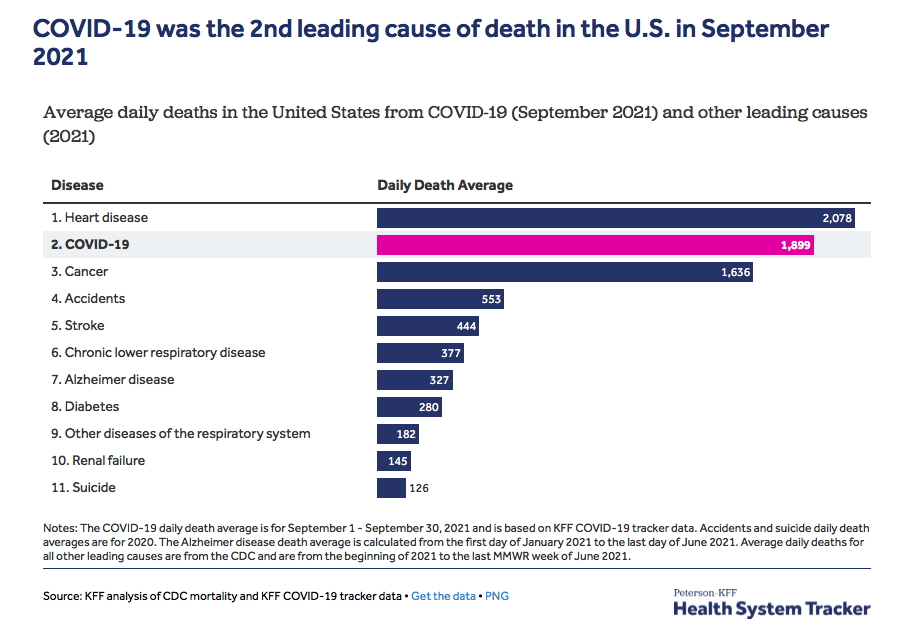
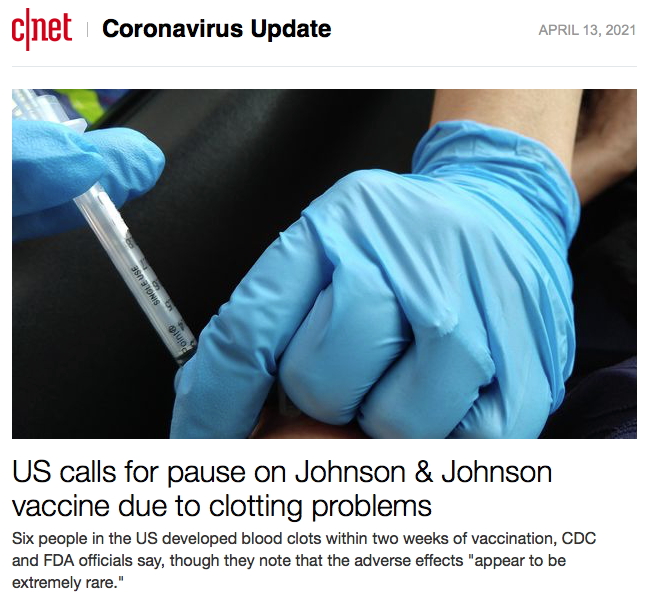

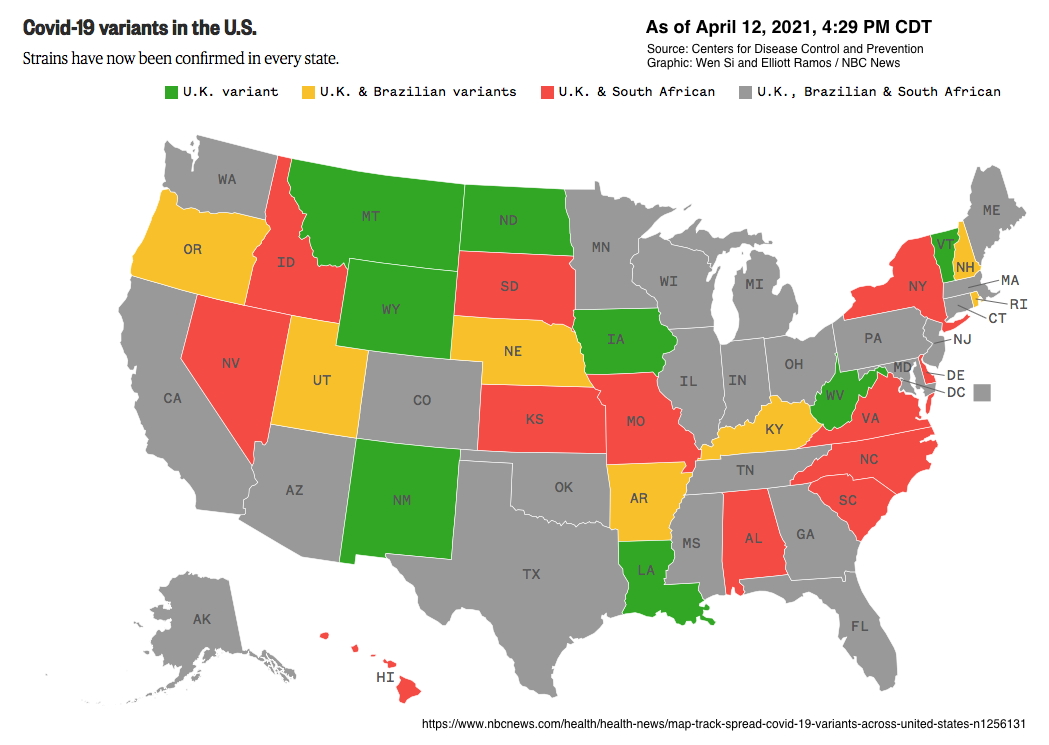
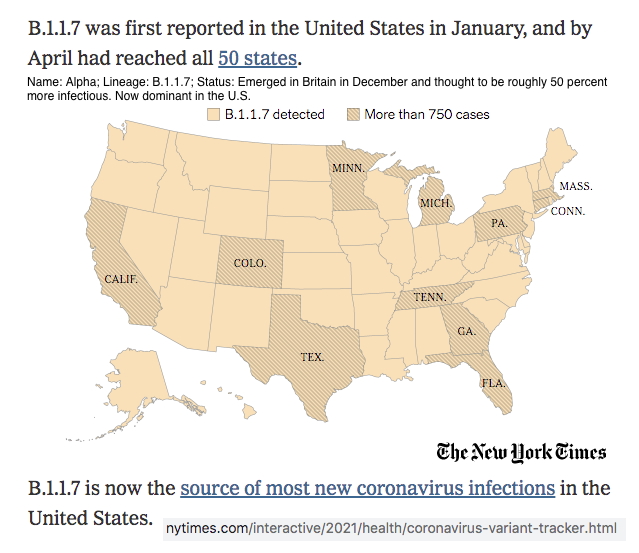
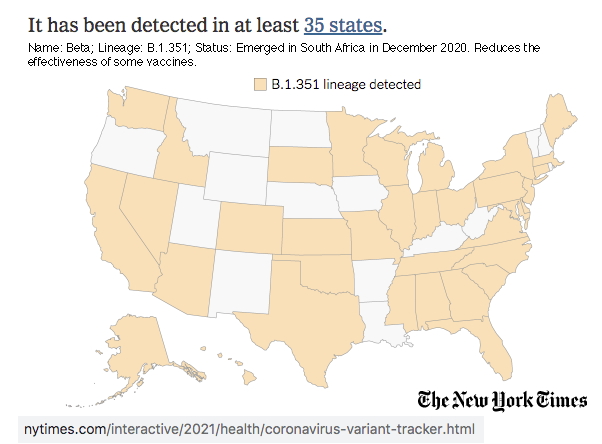
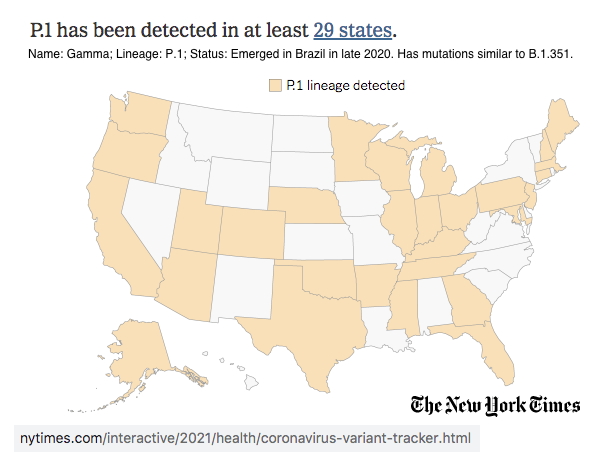
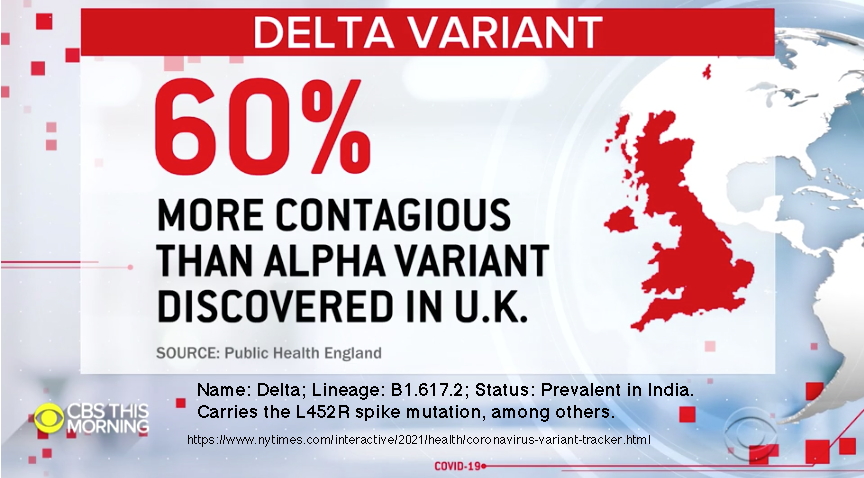


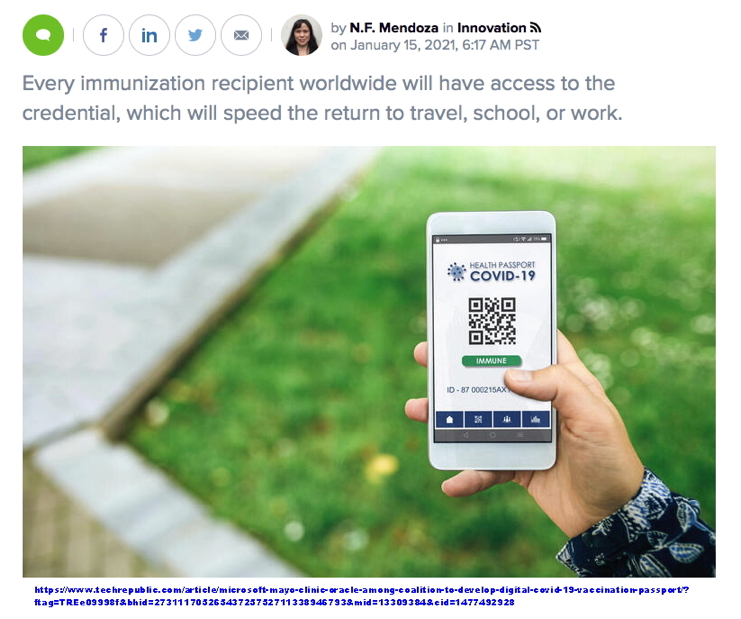

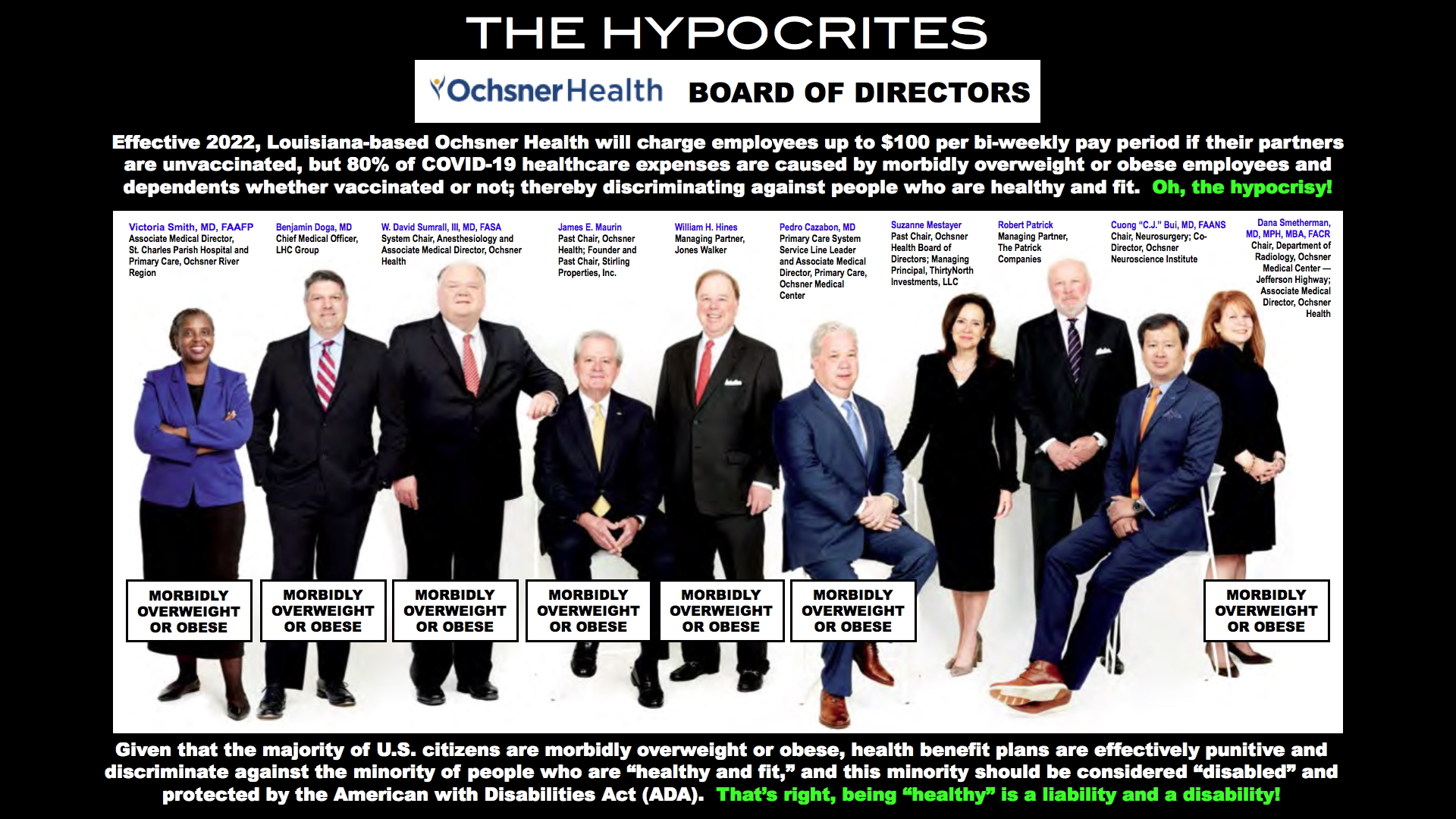

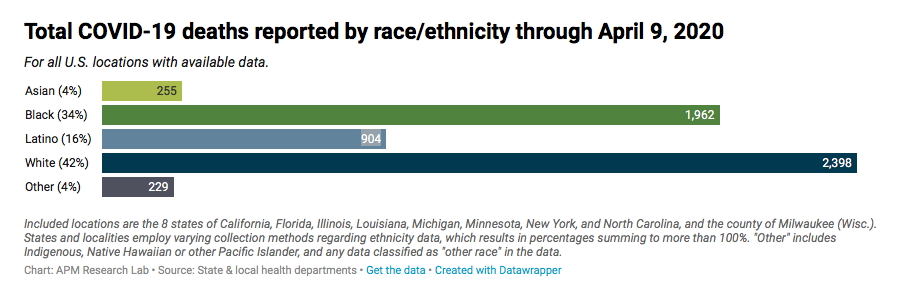
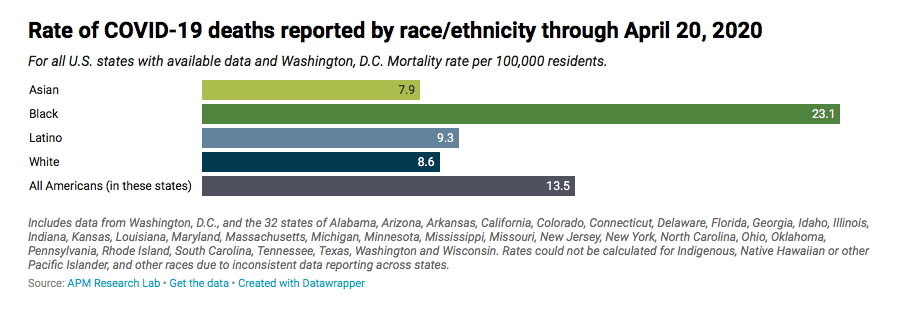
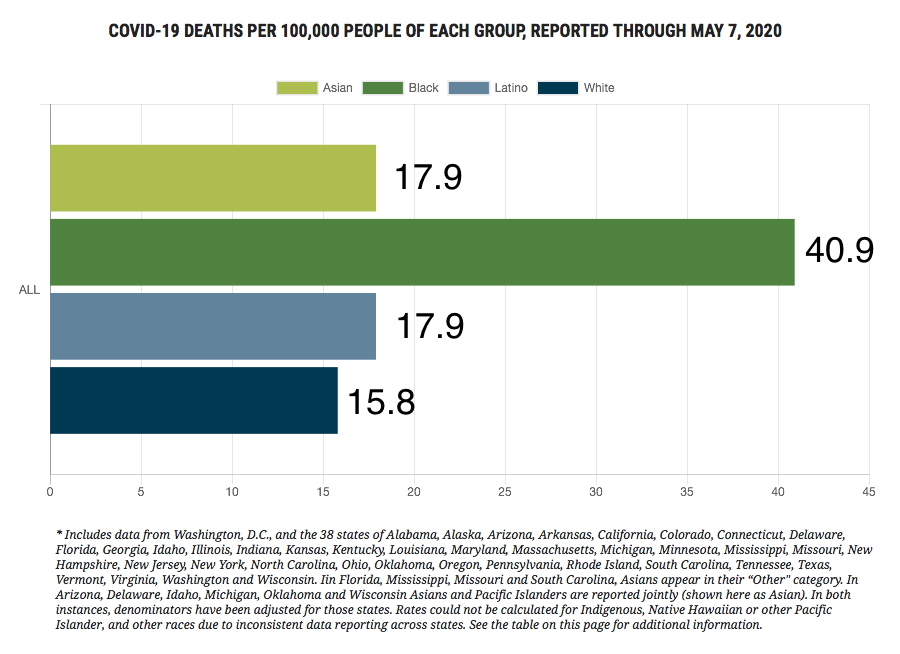
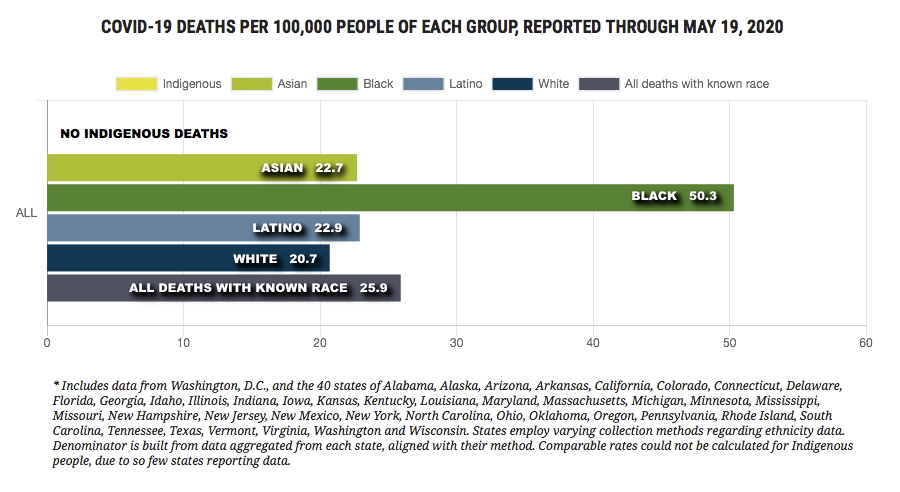
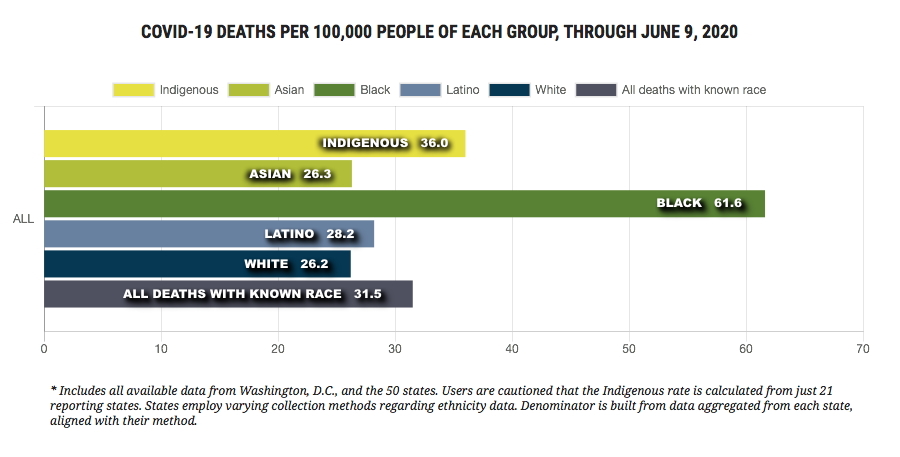
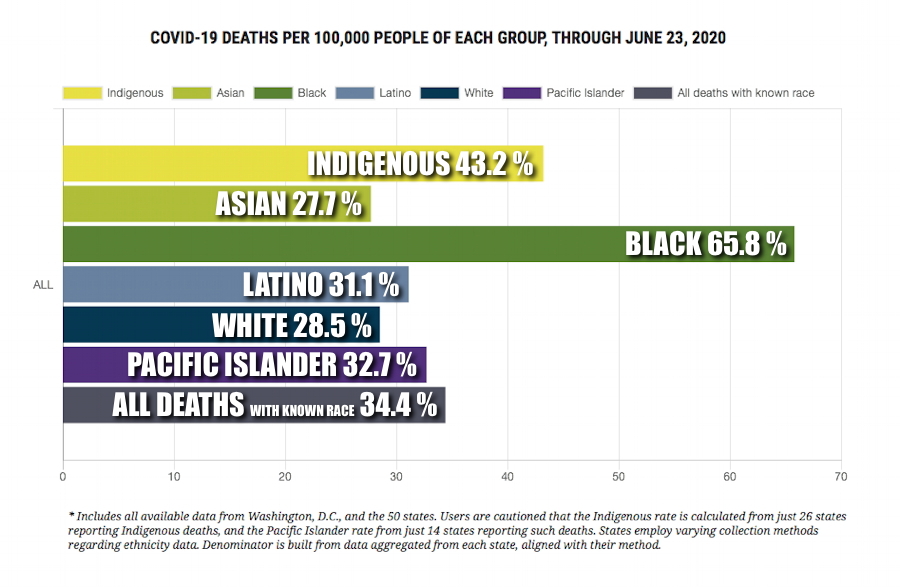
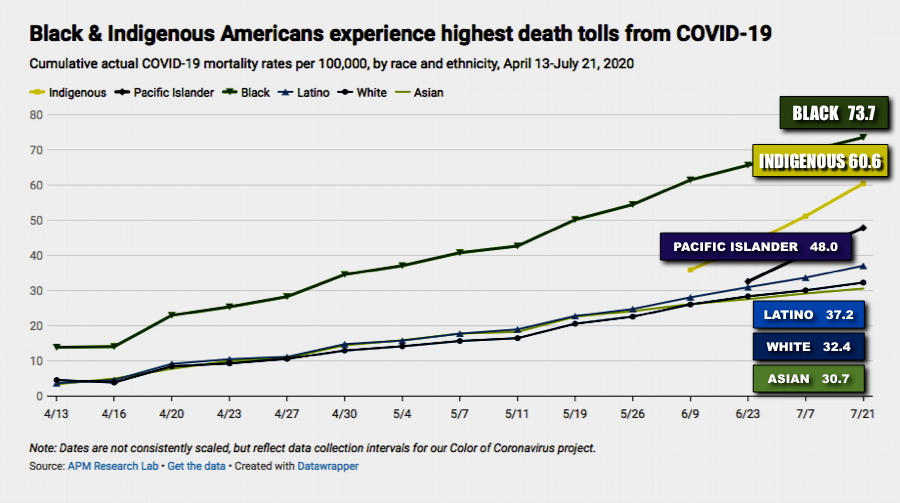
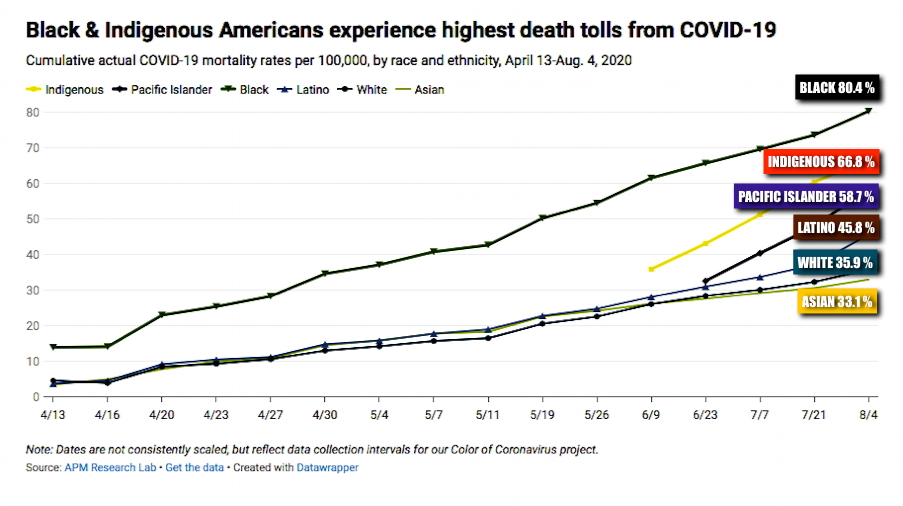
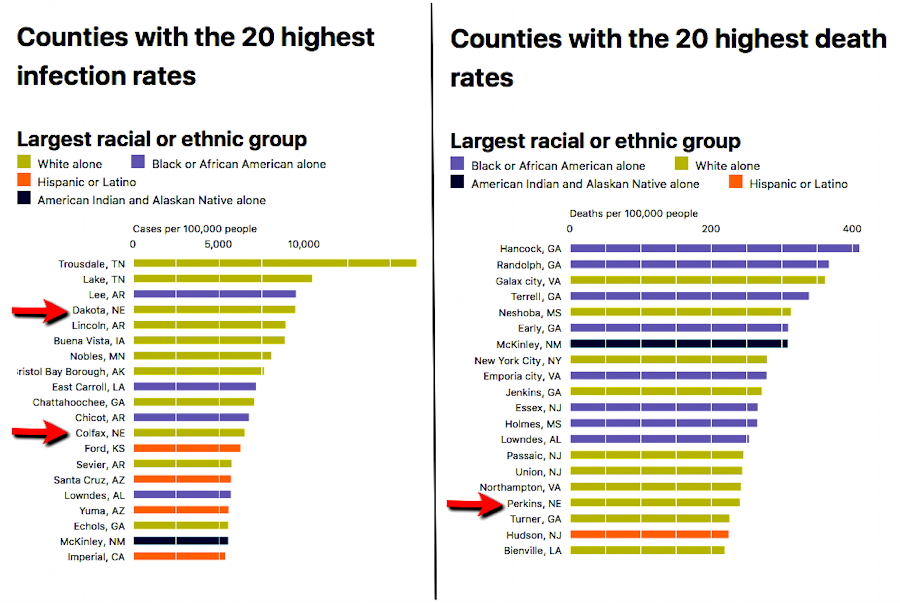
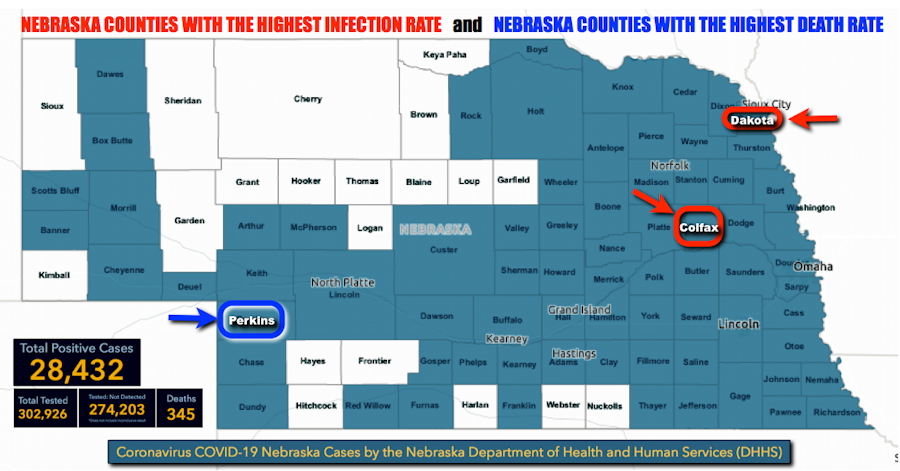
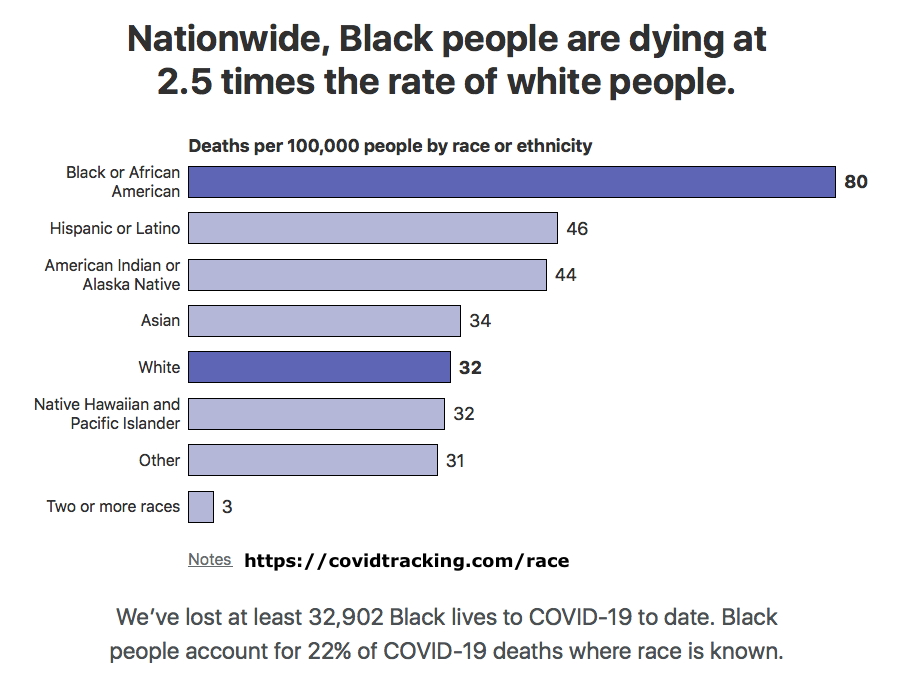
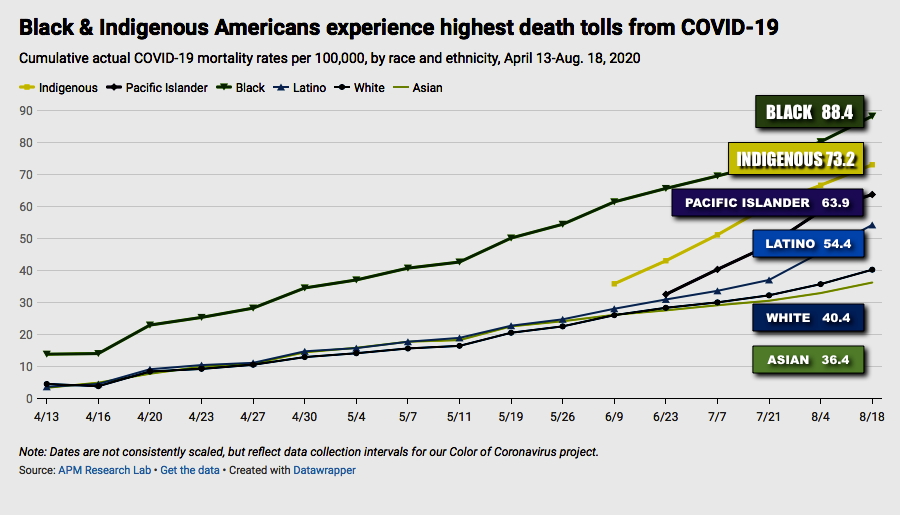
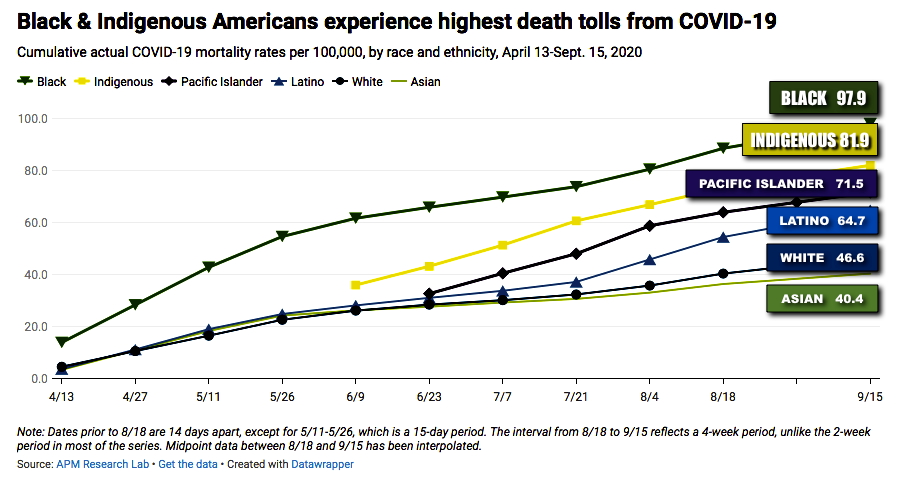
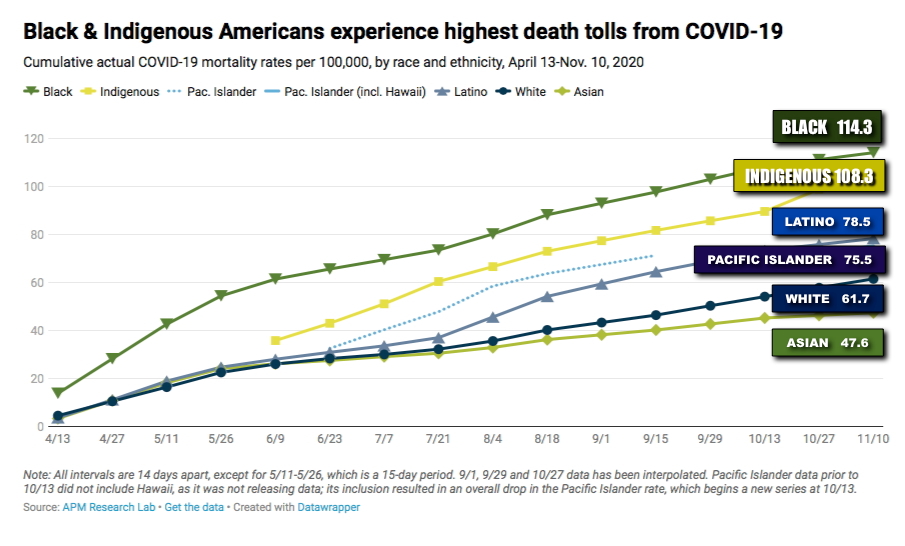
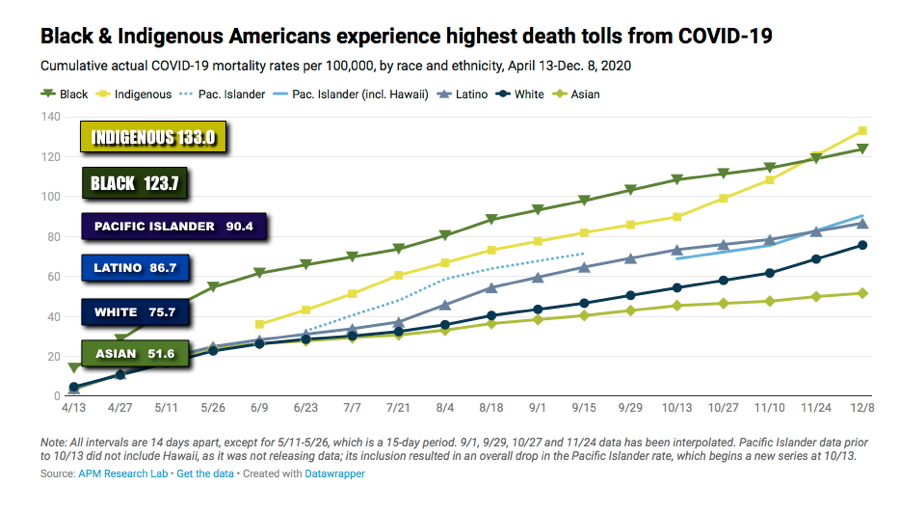
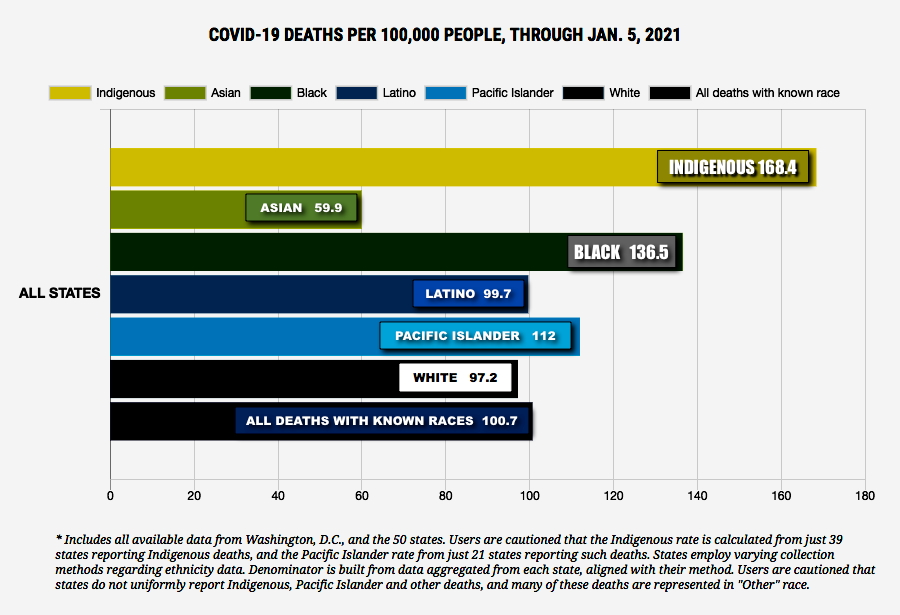
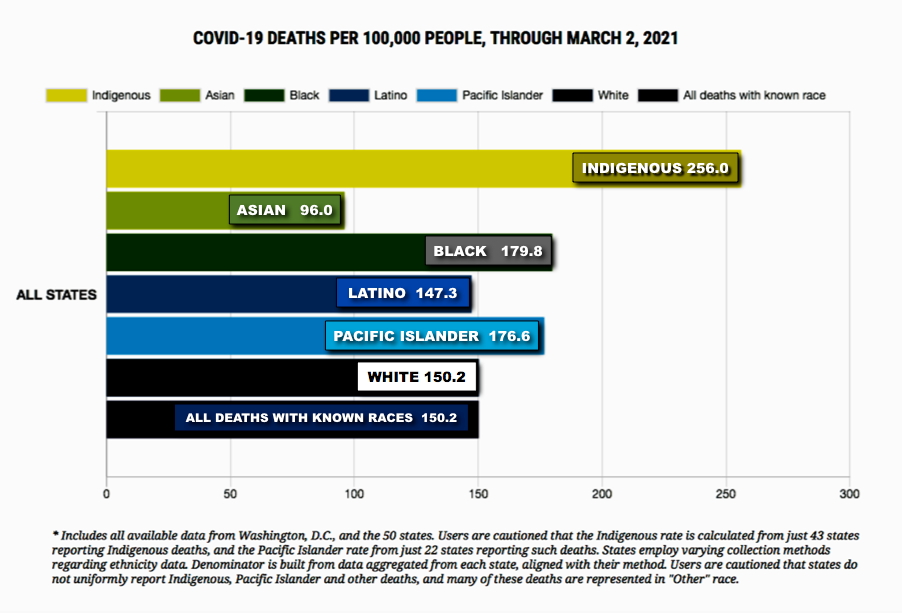
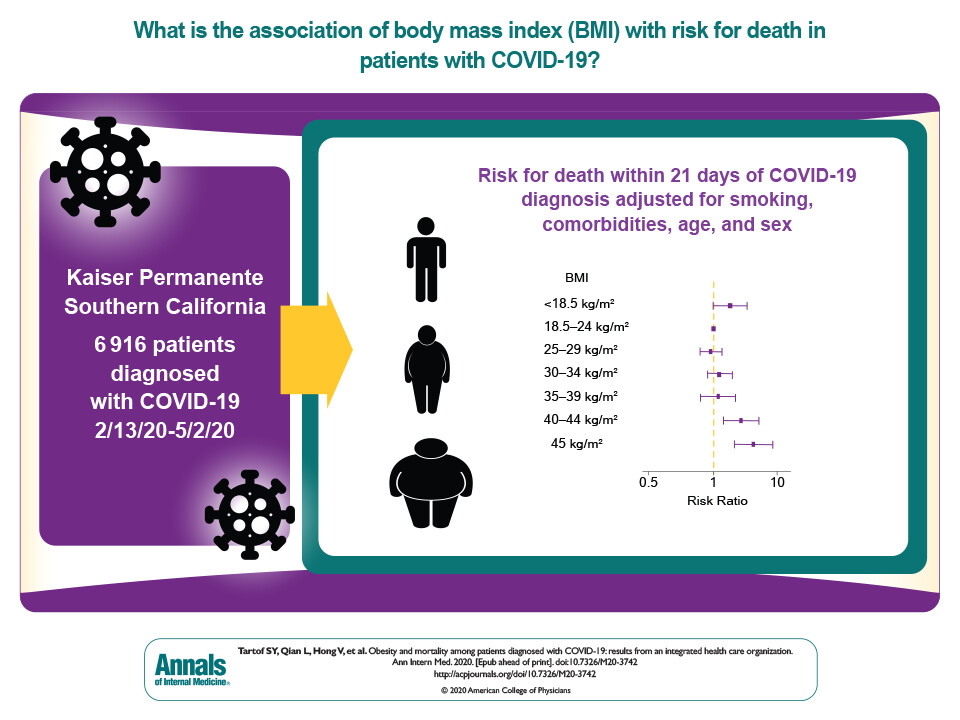
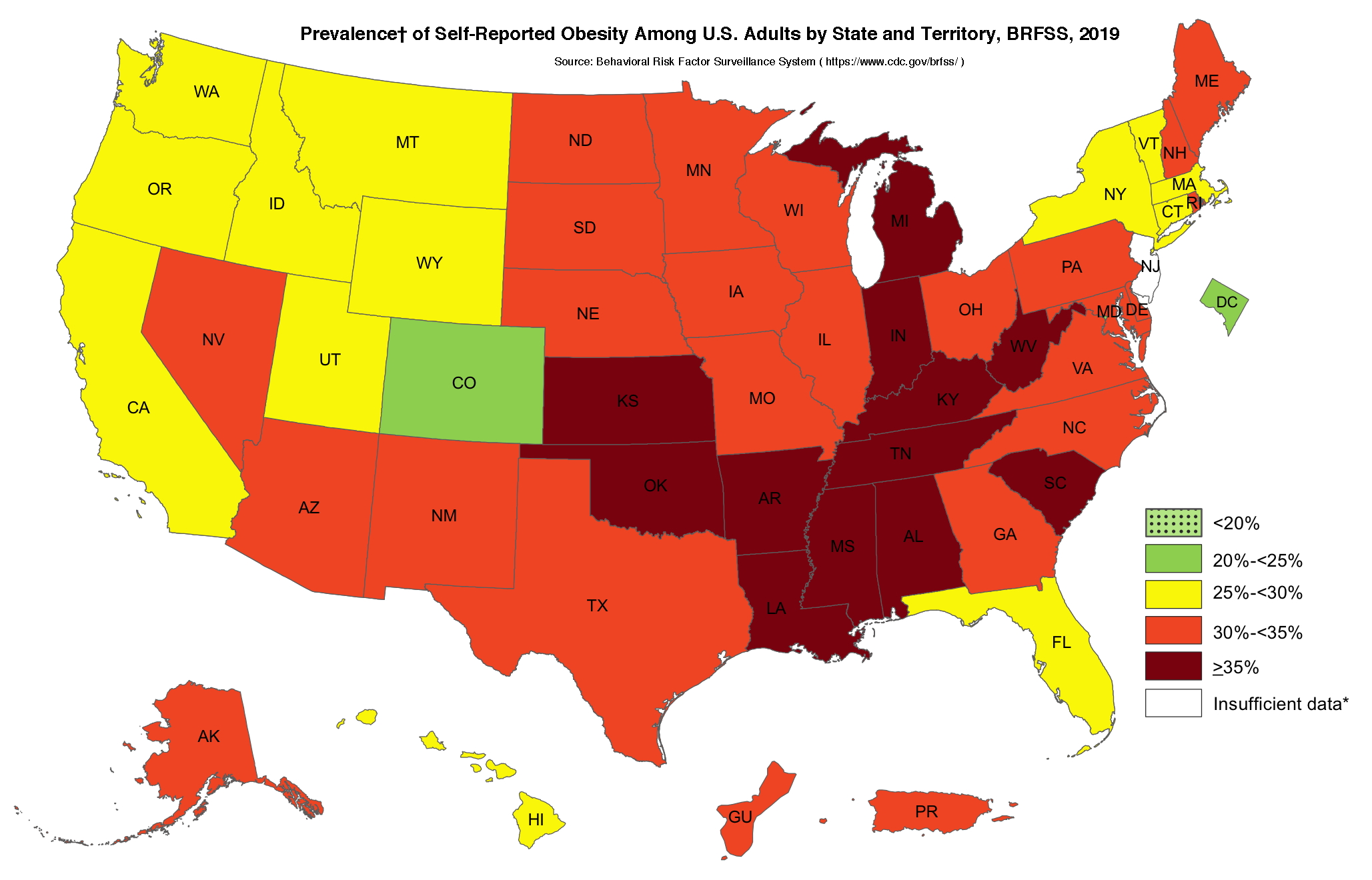











{kind=link}
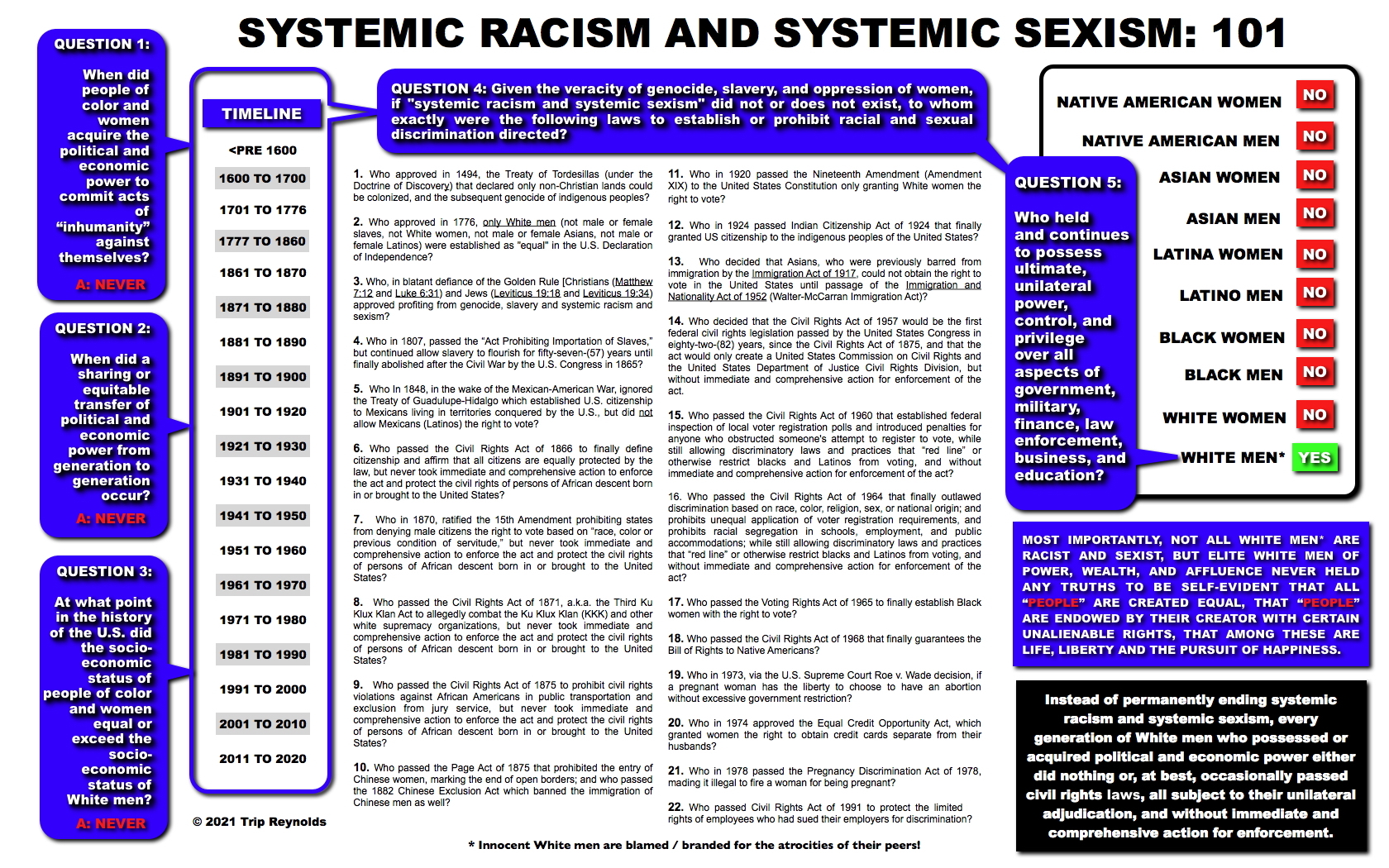{kind=link}